
Remember me

Multidrug-resistant micro-organisms (MDRO) have emerged globally as a significant public health concern. In 2019, the mortality attributed to MDRO in the entire WHO European region was 133,000 cases [1]. MDRO are also a pressing issue in Ukraine, with 48% of healthcare-associated infections (HAIs) caused by Enterobacterales resistant to third-generation cephalosporins and 17% of HAIs associated with resistance to carbapenems [2]. The European Centre for Disease Prevention and Control (ECDC) has warned that healthcare providers should be aware of MDRO in people presenting with traumatic wounds and that diagnostic procedures should be in place for identifying such organisms and preventing their spread [3]. Since March 2022, European countries including Denmark, Germany and the Netherlands reported an influx of MDRO from Ukrainian patients in national surveillance programs, leading to difficult–to-treat infections as described in several case reports [4,5,6,7,8,9,10].Here we report on the clinical and microbiological findings of a young Ukrainian soldier who was transferred to the trauma surgery department in a Dutch hospital. Informed consent for publication was obtained.
Case descriptionA young Ukrainian soldier was injured by a mine-blast on the Russia-Ukrainian battlefield, resulting in severe pelvic-perineal soft-tissue injury complicated by open pelvic and femoral fractures, intra-abdominal penetration injury and retroperitoneal pelvic bleeding, for which he underwent external fixation of the fractures and six laparotomic surgeries in a Ukrainian field hospital. During this admission, he received antibiotic treatment with at least meropenem, amikacin and colistin (no further details available). After a month, the patient was transferred to a regular Ukrainian hospital where he was treated for 90 days (no details available). He was then transferred to a trauma center in a Dutch hospital. The patient had a diverting colostomy and an external fixation of the hip and femur in place. Upon admission to our facility, he was placed on contact precautions and MDRO screening cultures were taken from multiple anatomical sites. Further surgical treatment consisted of removal of the external fixators, multiple wound debridements, a Girdlestone procedure at day 16 after transferal and vacuum assisted closure therapy.
The patient’s hospital course was complicated by three different HAI episodes with MDRO. Firstly, on day 2, while MDRO screening cultures were still pending, the patient developed a febrile episode, for which empiric treatment was started consisting of ceftazidime-avibactam, ciprofloxacin and gentamicin intravenously (IV); the central venous catheter (CVC) was removed. A single (peripheral) blood culture yielded an extensively drug-resistant (XDR) A. baumannii (Fig. 1A), culture of the catheter tip remained negative. Due to fast and complete recovery within a few hours after catheter removal despite inappropriate antibiotic treatment, antibiotic treatment was discontinued after three days. Final diagnosis was a possible CVC-related infection.
Fig. 1

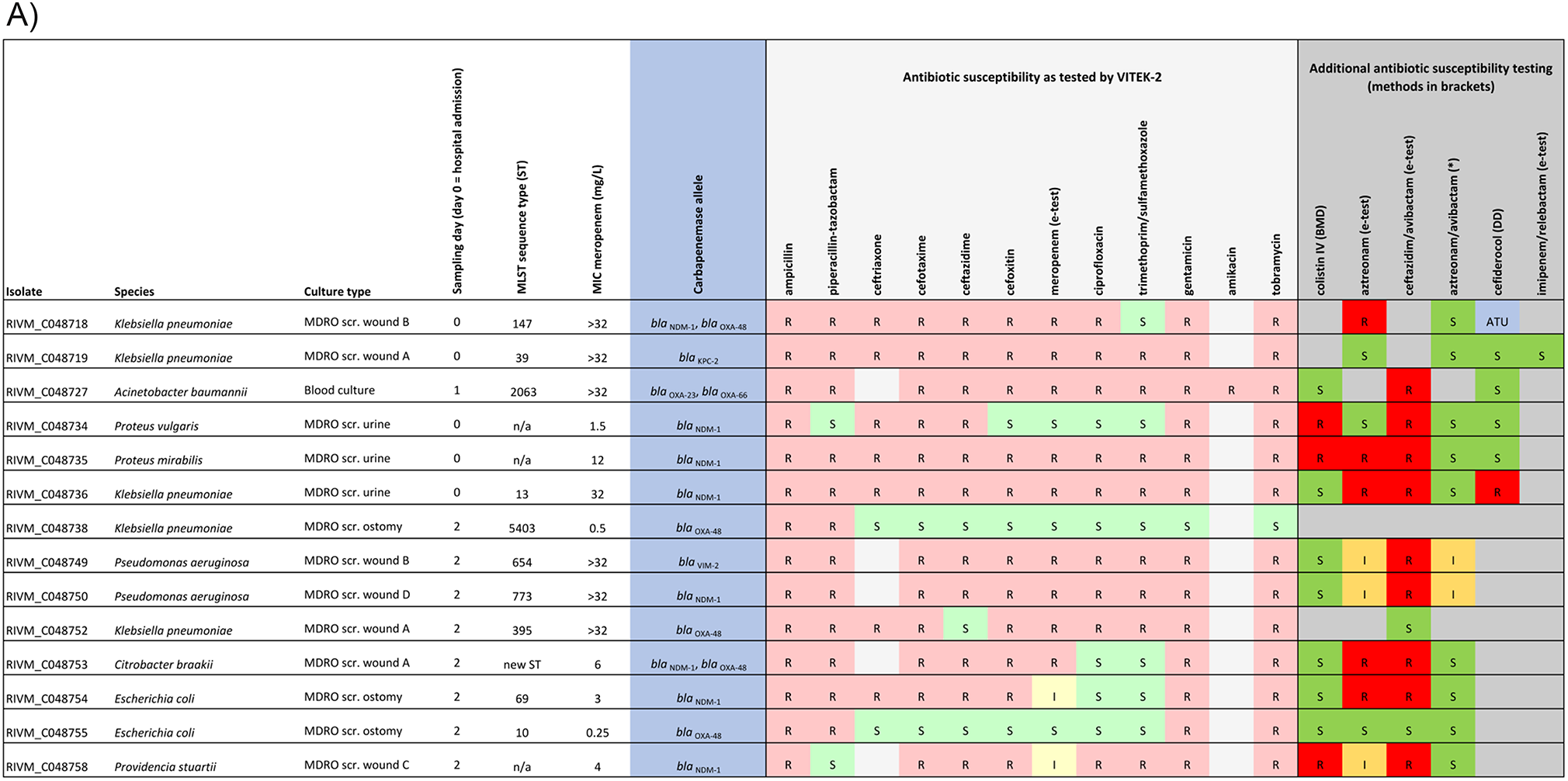
Genetic and phenotypic characteristics of the 14 MDRO and of complete blaOXA−48- and blaNDM−1-carrying plasmids. A) Genetic and phenotypic characteristics of 14 MDRO. Phenotypic testing results were interpreted according to EUCAST v13.1 guidelines. All isolates tested positive in the carbapenem inactivation method. Legend: * as determined by synergy between aztreonam with ceftazdime/avibactam (E-tests); ATU, area of technical uncertainty; BMD, broth microdilution; DD, disk diffusion; I, susceptible, increased exposure; IV, intravenous; MIC, minimum inhibitory concentration; MDRO scr., screening culture multidrug-resistant micro-organisms; MLST, multilocus sequence typing; R, resistant; S, sensitive. B) Characteristics of complete blaOXA−48- and blaNDM−1-carrying plasmids. Size is in base pairs and %G + C content is indicated. High similarity (≥ 90%) is indicated in red, while low similarity (≤ 10%) is indicated in blue. The resistome and plasmid replicons are depicted as black squares (100% identity to the reference based on ResFinder and PlasmidFinder) and grey squares (< 100% identity to the reference based on ResFinder and PlasmidFinder). If there is no grey/black square indicated, the resistance gene or replicon is absent
During the first week of admission, results from MDRO-screening became available, and yielded 11 carbapenemase-producing Enterobacterales (CPE), two carbapenemase-producing Pseudomonas aeruginosa (CPPA) (Fig. 1A), as well as the extensively drug-resistant (XDR) A. baumannii that had first been identified in the blood culture. The patient was not colonized with methicillin-resistant Staphylococcus aureus or vancomycin-resistant Enterococcus, as tested at admission according to national guidelines.
On day 22 of admission, the patient developed a second febrile episode, most likely due to a deep-seated wound infection. Treatment consisted of ceftazidime-avibactam + aztreonam, with addition of colistin IV for coverage of the different carbapenemase-producing isolates with which the patient was colonized, including metallo-β-lactamase (MBL) producing Gram-negative bacteria (Fig. 1A). Blood and other clinical cultures cultures remained negative and treatment was discontinued after 20 days. Third, on day 55 the patient developed fever and signs of a bacterial meningitis shortly after removal of a dislocated spinal catheter used for pain management. Empiric treatment consisted of ceftazidime-avibactam + aztreonam + vancomycin IV. Cerebrospinal fluid (CSF) culture yielded an XDR A. baumannii (phenotypically identical to the prior blood culture isolate Fig. 1A), upon which colistin both intravenously and intrathecally were added to the treatment, as well as minocycline orally; vancomycin was discontinued after three days. The patient fully recovered and after two weeks, and intrathecal treatment was discontinued. Systemic antibiotics were continued for another two weeks, because spinal epidural abscesses could not be excluded, as a MRI could not be performed due to in body embedded metal shrapnel. After 147 days in the Dutch hospital, the patient was discharged to a rehabilitation center.
Microbiology methodsScreening for MDRO was performed using flocked swab Amies medium (Copan Eswab), followed by non-selective enrichment using BHI broth and inoculation on selective agars: ETP-CLOX = ertapenem (0.25 mg/L), cloxacillin (400 g/L), vancomycin (32 mg/L); MacConkey-EbSA = ceftazidime / cefotaxim (1 mg/L), cloxacilline (400 g/L), vancomycin (32 mg/L); MacConkey-CI-TO/GE = ciprofloxacin (0.5 mg/L), tobramycin/ gentamicin (2 mg/L), vancomycin (32 mg/L) (Mediaproducts Groningen, the Netherlands). Screening breakpoints for carbapenemase-production according to national guidelines were: meropenem > 0.25 mg/L and imipenem > 1.0 mg/L (excluding Morganellaceae [Morganella spp., Providencia spp., Proteus spp.] and Serratia spp.). Each phenotypically unique Gram-negative isolate that was either carbapenemase positive (PCR in-house test; targets OXA-48/OXA-23, VIM, IMP-1/IMP-2, NDM, KPC) (n = 13) or phenotypically suspect for carbapenemase production with a negative in-house carbapenemase PCR (n = 1), was sent to the National Institute for Public Health and the Environment as part of the national CPE/CPPA/CRAB-surveillance program [11]. Meropenem E-test, carbapenem inactivation method (CIM), MALDI-TOF, lllumina next-generation sequencing (NGS) and Nanopore long-read sequencing were performed on the 14 isolates (BioProjects PRJNA903550, PRJNA1145137, PRJNA1020275). NGS data was used to determine MLST sequence type, to perform whole-genome MLST (wgMLST) analysis, to identify antimicrobial resistance genes by interrogating ResFinder and plasmid replicons using PlasmidFinder. Reconstruction of plasmids was performed by hybrid assembly using Unicycler of short-read and long-read sequencing data.
Microbiology resultsBased on MLST and wgMLST using specific in-house wgMLST schemes, 14 unique MDRO were identified with different MLST sequence types, and carrying six different carbapenemase genes. All phenotypically unique isolates are presented with their first day of isolation in Fig. 1A, but were often found in multiple body sites. All isolates phenotypically produced at least one carbapenemase as assessed by the CIM, and had MICs for meropenem ranging from 0.25 to > 32 mg/L (Fig. 1A). The blaNDM-1 gene was the most frequently identified carbapenemase allele, found in eight CPE/CPPA strains, while the blaOXA-48 gene was carried by five different CPE isolates. Three strains carried two carbapenemase genes. The five CPE carrying blaOXA-48 yielded five circular assemblies of which three unique and non-related (% identity < 23%) plasmids with different plasmid sizes, varying %G + C content, and plasmid replicons (Fig. 1B). Two large OXA-48-carrying plasmids in Klebsiella pneumoniae and Escherichia coli were highly similar (99%), had highly similar plasmid size, %G + C content, resistome and IncHI1B(pNDM-MAR)-like plasmid replicons. Eight CPE/CPPA carrying blaNDM-1 yielded five circular assemblies included in the analysis, of which three carried nearly identical blaNDM-1-carrying multi-drug resistance plasmids of 157.1 kb with a %G + C of 51.98% and an IncC replicon yet detected in different species: an XDR Providencia stuartii and Citrobacter braakii and highly-resistant E. coli. In four isolates, no circular plasmid assemblies were obtained.
Comments (0)