The results of our study align with previously published reports on the clinical features and imaging findings of HFRS [1, 2, 10,11,12,13]. Febrile manifestations, abdominal pain, back pain, and oliguric AKI were frequently observed in our study population, consistent with earlier studies [1]. Regarding imaging findings, juxta-renal involvement and fluid third-spacing were prominent features [12, 13]. While renal swelling is a recognized imaging finding in HFRS, no standardized criterion exists for determining nephromegaly based on pole-to-pole kidney length. In our study, the mean pole-to-pole lengths of the right and left kidneys were 114.8 mm and 118.3 mm, respectively, which are smaller than the corresponding measurements of 125.7 mm and 127.8 mm reported in a Belgian hospital [13]. Variations in body habitus and ethnicity between the study populations may have contributed to this discrepancy.
The CT severity score was developed based on careful observation of common imaging features previously described in the literature [10,11,12,13]. Notably, the features classified as juxta-renal findings appeared in a stepwise progression: all patients with anterior pararenal fat stranding also demonstrated pararenal fascia thickening, and all with pararenal fascia thickening exhibited perirenal fat stranding. This unique imaging spectrum underscores the progressive nature of juxta-renal involvement, ranging from isolated perirenal fat stranding to the combined presence of all three findings.
Although the CT severity score was developed solely based on imaging findings, it demonstrated moderate to strong correlations with laboratory markers of inflammation (white blood cell count), thrombocytopenia (platelet count), and proteinuria (uPCR, albumin, and total protein). This indicates that the CT severity score effectively reflects the underlying disease process. Furthermore, previous studies have identified hypoalbuminemia, proteinuria, and thrombocytopenia as markers of disease severity, providing additional validation for the CT severity score as a reliable indicator of the clinical manifestations of HFRS [5, 6, 8, 9].
However, the components of the CT severity score are highly nonspecific imaging features, warranting careful interpretation. Fluid third-spacing can result from a variety of causes, including malignancy, inflammation, renal insufficiency, heart failure, and portal hypertension [18]. To enhance the specificity of the CT severity score, fluid third-spacing was excluded when juxta-renal findings were absent. Nevertheless, juxta-renal findings themselves can also arise from diverse etiologies, such as renal inflammation, infection, systemic diseases, fluid overload, or bladder outlet obstruction [19, 20]. Notably, the observation that juxta-renal findings can result from fluid overload raises the possibility that the CT score’s prognostic value may, in part, reflect the detection of aggressive resuscitation efforts in patients already experiencing clinical deterioration. Severe fluid overload is also a major indication for renal replacement therapy (RRT) [21]. Ideally, the confounding effect of fluid overload should have been accounted for; however, due to the retrospective nature of this study, precise input and output monitoring before and during hospitalization was unavailable for most patients. This limitation represents a significant drawback of our study. Additionally, our study population consisted exclusively of young male military personnel in their twenties, which may have led to an overestimation of the utility of the CT severity score. For broader generalizability, further validation studies are needed, incorporating patients of varying ages and genders.
In our study population, the CT severity score demonstrated a significant correlation with nephrotic range proteinuria. Hantavirus species that cause HFRS have a tropism for renal capillaries [1, 2, 22]. After entering the endothelial cells of renal capillaries, the virus activates various pathways to release vasoactive factors, resulting in increased vascular permeability, platelet activation, and an overreacting host immune response. In addition to endothelial cells, podocytes and tubular epithelial cells can also be infected by the virus, resulting in massive proteinuria [22]. The degree of proteinuria is known to be related to the severity of the disease, but excess protein in the urine itself can also cause nephrotoxicity and exacerbate kidney damage [5, 14, 17, 22]. Thus, it is noteworthy that the CT severity score correlates well with the degree of proteinuria, reflecting its potential as a reliable indicator of disease severity.
There are several reasons why RRT was selected as a clinical outcome. First, RRT is generally indicated for severe AKI, so the use of RRT itself was considered to indicate serious renal damage [14, 21, 23]. Second, there are previous reports claiming that the optimal timing of RRT improves prognosis in patients with severe AKI compared with delayed RRT application [23]. Therefore, using the CT severity score to predict future RRT requirements in advance has the potential to help physicians prepare for RRT at the appropriate time, thereby improving patient prognosis. Third, regardless of the timing of RRT, access to this advanced treatment is often unavailable in resource-limited hospitals. Early risk stratification using the CT severity score could help identify patients likely to require RRT, allowing for timely transfer to referral hospitals before clinical deterioration occurs, ultimately benefiting patient prognosis.
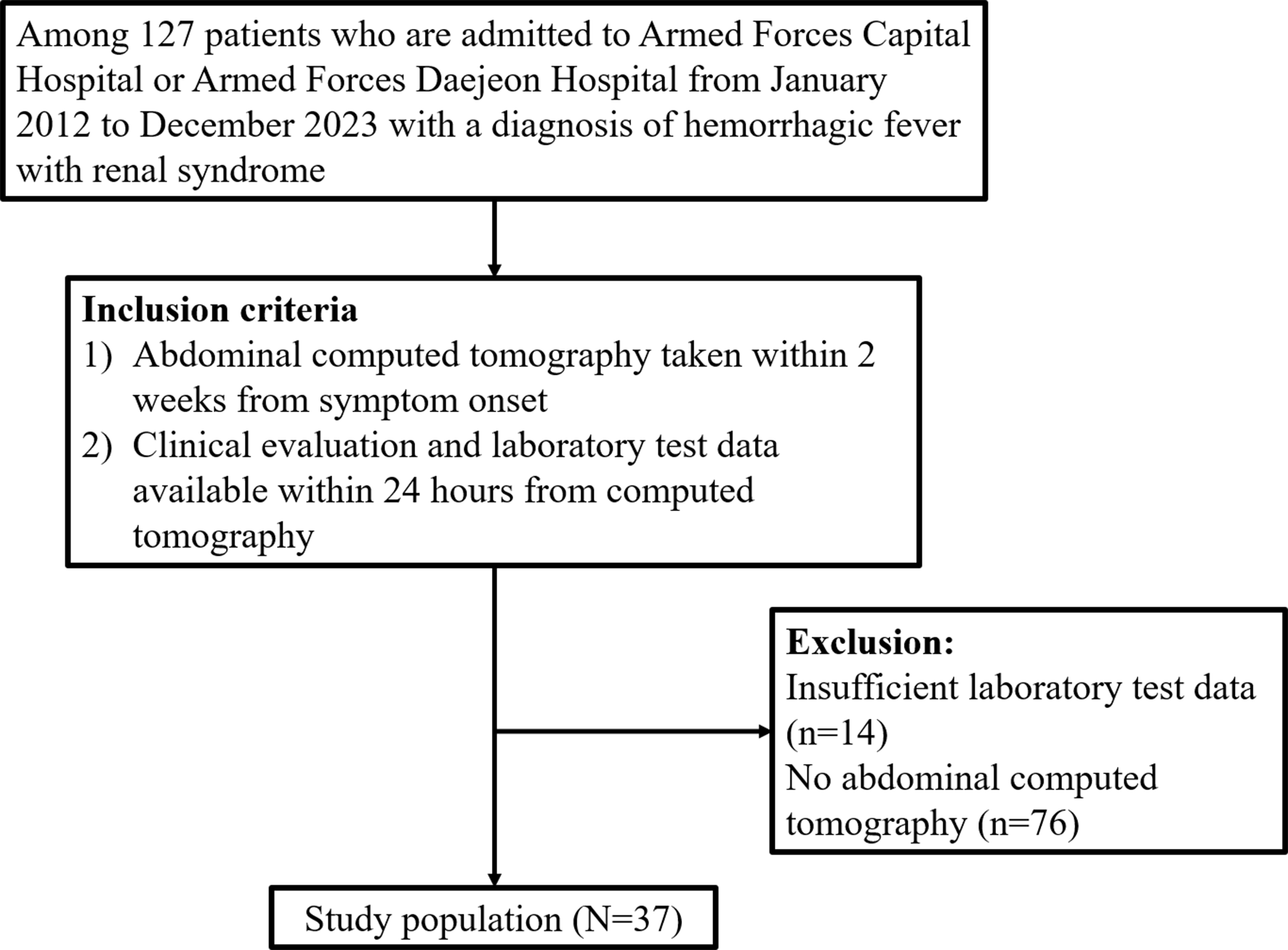
In previous studies on prognostic factors in HFRS that included more than 100 patients, several laboratory variables—C-reactive protein, total bilirubin, albumin, thrombocytopenia, and proteinuria—were reported as significant prognostic markers [6, 7, 9]. However, in our study, these variables did not demonstrate statistically significant associations with HFRS prognosis in univariable analysis. Given the relatively small sample size of our study (n = 37), it is plausible that repeating the analysis in a larger population could yield results more consistent with previous literature, where a greater number of clinico-laboratory variables reached statistical significance in univariable analysis. A larger study would also allow for a multivariable model with multiparametric adjustment, which could help determine whether the CT severity score remains an independent prognostic indicator even after controlling for other significant factors. Therefore, further research with a larger population is necessary to validate these findings.
Abdominal CT is not routinely performed in patients with suspected HFRS, likely due to insufficient evidence supporting its diagnostic or prognostic value to justify the radiation exposure and, especially in the case of contrast-enhanced studies, the potential nephrotoxicity of iodinated contrast agents [14]. This study, however, indicates that the CT findings identified as prognostically significant can be evaluated without the use of iodinated contrast agents. In our study population, more than half of the patients underwent contrast-enhanced CT. Due to the retrospective nature of this study, it was not possible to determine a clear justification for the use of contrast agents. Even if contrast administration was unnecessary, our findings demonstrate the potential utility of noncontrast CT in HFRS management. With modern dose-reduction strategies, low-dose noncontrast abdominal CT could be a reasonable option for evaluating patients with or suspected of having HFRS [24, 25].
This study has several limitations that should be considered. First, the retrospective design may have introduced selection biases. The absence of randomization and standardized imaging protocols could have affected the generalizability of the results. Second, the study population consisted exclusively of young male military personnel, which may limit the applicability of the findings to broader populations, including females, older adults, and individuals with diverse comorbidities. The fact that overall patient outcomes were very good compared to the known high mortality rate of HFRS would probably be attributable to the extremely biased study population [1, 2]. Third, only 24.3% (9 out of 37) of the study population had a definitive identification of the causative pathogen through polymerase chain reaction, confirming Hantaan virus disease. Immunofluorescence assay, used for the remaining patients, cannot differentiate between viruses within the orthohantavirus genus. South Korea is an endemic area for both Seoul virus and Hantaan virus [2]. Potential differences in imaging findings and outcomes between different viruses were not addressed in the current study [1, 2]. Fourth, while the CT severity score demonstrated significant correlations with markers of inflammation, thrombocytopenia, and proteinuria, its nonspecific imaging features require cautious interpretation, as these findings can also arise from non-HFRS conditions [18,19,20]. Finally, the small sample size may have limited the statistical power. Future studies involving larger, more diverse populations and prospective designs are needed to validate and refine the CT severity score for broader clinical application.
In conclusion, this study introduces a novel CT severity score for HFRS that correlates with degree of proteinuria and the need for renal replacement therapy. The score’s reliance on noncontrast imaging makes it a safer option for risk stratification, particularly in resource-limited settings. Further validation in larger, and more diverse populations is needed to confirm its clinical utility.

Comments (0)