Setting
The study was conducted in an adult major referral hospital in metropolitan Melbourne, Victoria, with an annual emergency department (ED) attendance of approximately 65,000 patients. The hospital provides state services for major trauma, burns, hemophilia, cystic fibrosis, heart and lung transplants, HIV, and adult hematological malignancies.
Design: A retrospective cohort study was conducted using explicit chart review.
Inclusion criteria
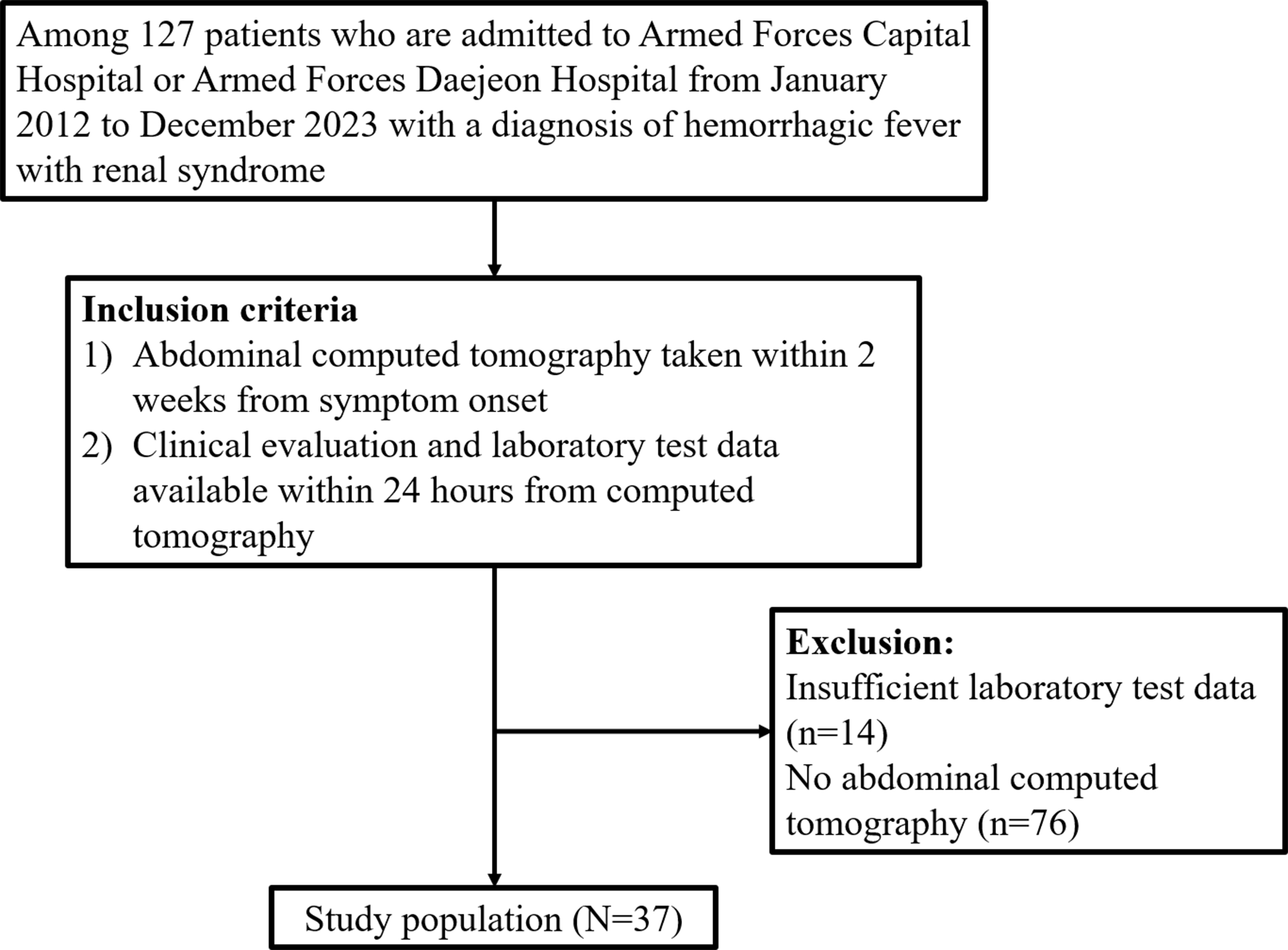
We included all adult patients who were investigated with a CXR in the ED between 01 Jan 2022 and 31 Dec 2022.
Exclusion criteria
The exclusion criteria consisted of patients who were under 18 years old, patients with more than one CXR during their presentation, patients without chest pain, patients with a traumatic etiology of chest pain, and patients without any medical history documented.
Data extraction
Data were extracted from the electronic medical record system using explicit chart review by a single investigator (AL). Data on demographics, presenting vital signs, hemoptysis, chest auscultation findings (diminished lung sounds, rales, wheezes), and history of venous thromboembolic disease (VTE), chronic lung diseases (including chronic obstructive pulmonary disease, asthma, cystic fibrosis, idiopathic pulmonary fibrosis, interstitial lung disease, history of lung transplant), heart failure, and smoking were extracted.
Past medical history and chest auscultation findings were categorized into present or absent. Smoking history was categorized as non-smoker, ex-smoker, or current smoker. Vital signs were categorized into abnormal or normal, based on the Royal Prince Alfred Hospital patient observation vital signs policy [14]. A respiratory rate of 12–20 breaths per minute, heart rate of 60–100 beats per minute, systolic blood pressure of 90–129 mmHg, temperature of 36.5-37.2oC, and oxygen saturations of 97–100% were considered normal [14].
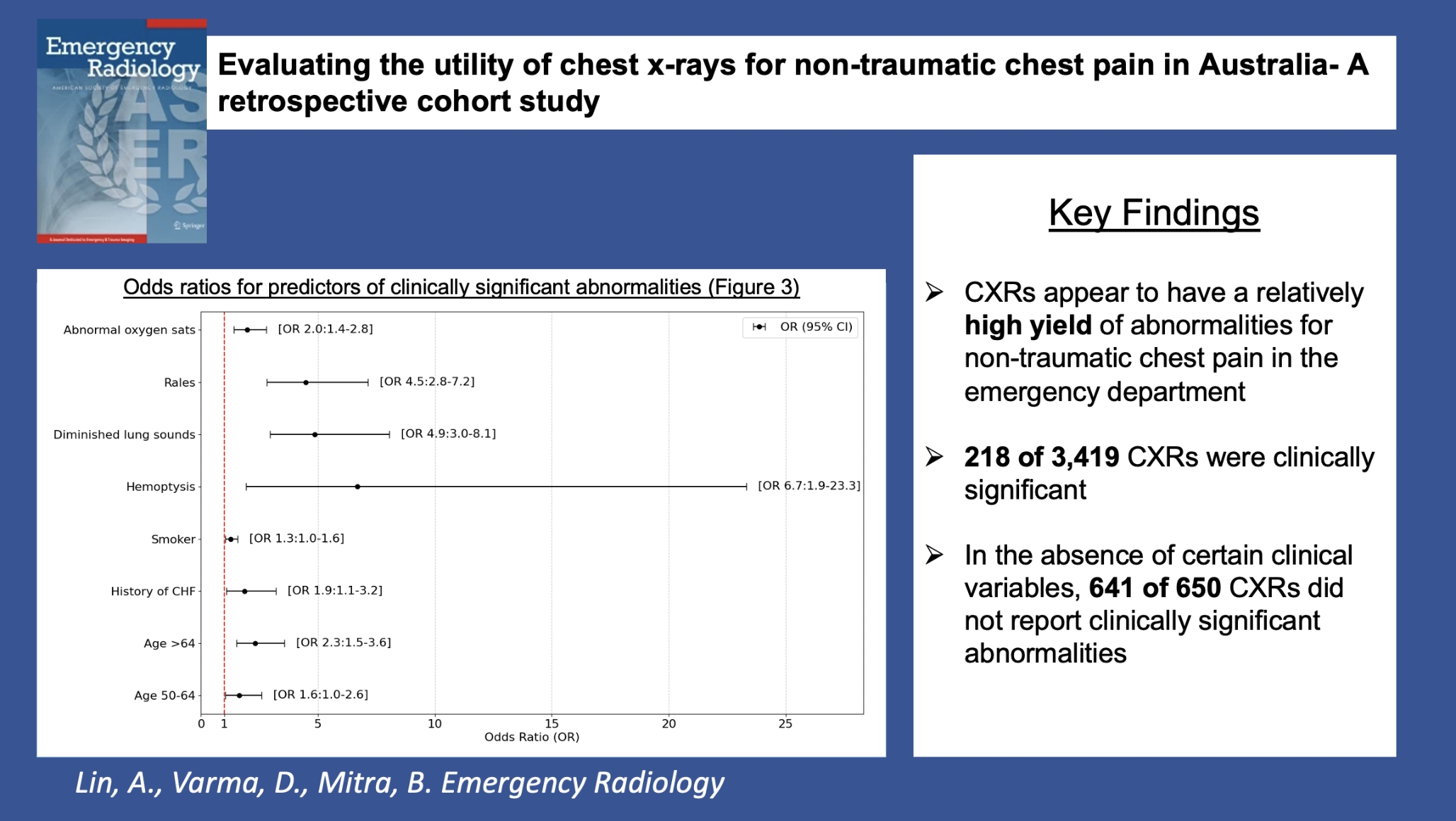
Radiology reports were extracted and CXRs were subgrouped into those with abnormalities reported and compared to those without. CXRs with abnormalities were subgrouped into those that were clinically significant and compared to those that were not. Overt signs of heart failure, consolidation, masses, and fractures that were likely to change management were considered to be clinically significant. Where signs of heart failure or infection were reported to be subtle, medical records were further reviewed to extract data on whether the abnormality had changed the clinical management of the patients. Specifically, the initiation of acute heart failure therapy or antibiotic therapy in the ED was considered to be clinically significant.
Statistical analysis
All data were summarized using counts (proportions) and differences were assessed using the chi-square test. The association of abnormal and clinically significant abnormal CXRs with clinical characteristics were assessed using univariable logistic regression analysis. Following this, a multivariable logistic regression model was developed with backward elimination. Results were reported using odds ratios and adjusted odds ratios with 95% confidence intervals. A p-value of < 0.05 was defined to be statistically significant.
Post-estimation testing was performed for the multivariable regression model using the Hosmer-Lemeshow test and variance inflation factor (VIF). The Hosmer Lemeshow test identifies the goodness of fit of the collected data to the model, and the VIF measures the levels of multicollinearity within the model.
All analyses were performed using Stata v18.0, College Station, TX, USA.
Ethics
The study was approved by the Alfred Hospital Human Research Ethics Committee. The requirement to seek informed consent from patients was waived by the ethics committee.

Comments (0)