
Remember me
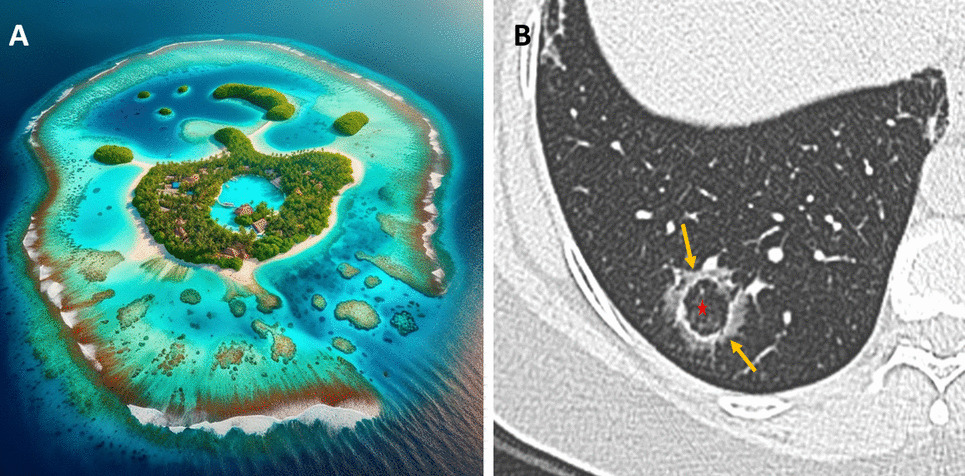
The reverse halo sign (RHS), also known as the “atoll sign,” is defined by a central area of ground-glass opacity (GGO) encircled by a denser rim of consolidation (Fig. 1) [1]. Increased awareness of the RHS has shown that a wide range of pulmonary conditions can present with this pattern [1,2,3]. In the emergency setting, accurately distinguishing these entities on chest CT requires integration of imaging findings with the patient's clinical presentation, laboratory data, immune status, and relevant history. This article provides an overview of the major causes of the RHS and essential CT findings.
Fig. 1
A Atoll: A ring-shaped coral reef or island. B Atoll Sign: The central area of ground-glass attenuation represents alveolar septal inflammation (Star), while the peripheral consolidation corresponds to inflammatory tissue (arrows)
Infectious causesBacterial pneumoniaBacterial pneumonia may manifest a RHS during the organizing phase of lung injury. Histopathologically, the central GGO corresponded to residual inflammatory exudates, while the peripheral rim of consolidation reflected the ongoing organization of the infection. Bacterial pneumonia can be distinguished from other causes of the RHS by integrating the patient's clinical context with its non-specific CT features. In bacterial pneumonia, including tuberculosis, the RHS typically appears during the evolving phase of the infection, characterized by a smooth, uniform rim of consolidation with surrounding GGO and ipsilateral pleural effusion (Figures 2 and S1). However, imaging findings may vary based on the patient’s immune status (Figure 3) [4].
Fig. 2
A Initial axial chest CT image demonstrates focal consolidation within the right lower lobe in a patient with COPD presenting with fever and cough. Sputum culture confirmed Streptococcus pneumoniae infection. B Axial and (C) coronal chest CT images obtained two weeks later reveal the development of the reverse halo (atoll) sign at the site of the prior consolidation
Fig. 3
A Axial and (B) coronal chest CT images of a patient with oral squamous cell carcinoma and immunosuppression demonstrate bilateral lower lobe and lingular consolidative pulmonary opacities. The left lower lobe and lingular opacities exhibit the reverse halo (atoll) sign (arrows). Sputum culture confirmed Staphylococcus aureus infection
Fungal infectionsFungal pathogens such as mucormycosis and aspergillosis can give rise to the so-called “bird’s nest” variant of the reversed halo (atoll) sign [1,2,3,4]. The “bird’s nest” pattern in fungal infections is marked by irregular, intersecting lines within the central area (Fig. 4). These opportunistic infections are particularly prevalent in immunocompromised or diabetic patients. In mucormycosis, the central GGO with intersecting lines often represents necrotic tissue, while the peripheral rim corresponds to inflammatory or fibrotic changes. Early detection of this pattern is critical because mucormycosis requires urgent and aggressive antifungal therapy, and delays in diagnosis can have dire consequences. Although the imaging appearance of aspergillosis may overlap with that of mucormycosis, subtle differences along with clinical cues (including specific risk factors and serologic tests) can help distinguish these entities [3, 4].
Fig. 4
A Coronal and (B) axial chest CT images of a patient with acute myeloid leukemia (AML) demonstrate a right lower lobe peripheral pulmonary opacity with a bird’s nest sign (arrows). This finding represents a reverse halo sign characterized by irregular and intersecting lines or stranding within an area of ground-glass opacity, indicative of invasive fungal infection. The patient was subsequently diagnosed with mucormycosis
Viral PneumoniaA variety of viruses—including influenza, respiratory syncytial virus (RSV), cytomegalovirus (CMV), and SARS-CoV-2 (COVID-19)—may demonstrate the RHS on CT imaging (Figs. 5, 6, and S2) [4, 5]. In viral pneumonia, the central GGO reflects inflammatory changes triggered by viral injury, while the surrounding consolidation indicates the host immune response. For example, in COVID-19 pneumonia, the RHS typically appears during the later or resolving stages of infection and may signal the development of post-inflammatory fibrosis [5]. Unlike bacterial or fungal infections, viral pneumonia is usually accompanied by a clinical history of recent viral exposure, fever, and cough, with laboratory findings that often include lymphopenia rather than the neutrophilia seen in bacterial infections [3,4,5].
Fig. 5
Examples of bilateral, multifocal atoll sign (arrows) in patients with (A–C) influenza pneumonia (H1N1). The images demonstrate multiple areas of ground-glass opacity surrounded by a peripheral rim of consolidation, characteristic of the reverse halo sign
Fig. 6
Examples of the atoll sign (arrows) in a patient with (A–C) COVID-19. The images demonstrate multiple areas of ground-glass opacity (GGO) surrounded by a peripheral rim of consolidation, characteristic of the reverse halo sign. Note the presence of scattered areas of GGO throughout the lungs
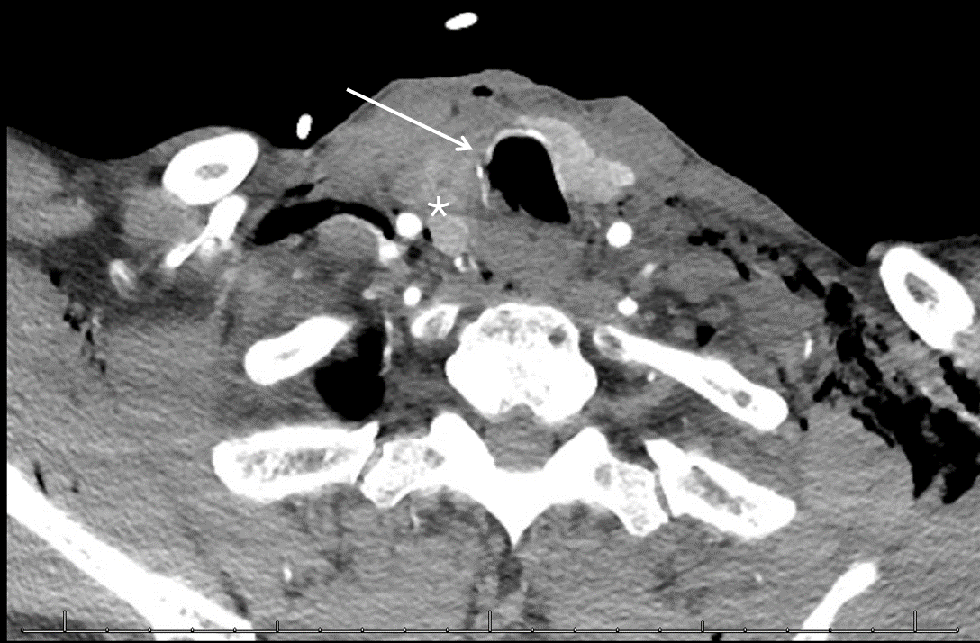
Parasitic infectionsPulmonary paragonimiasis, caused by the lung fluke Paragonimus spp., can occasionally present with the RHS in association with pleural effusion/thickening or pneumothorax (Fig. 7) [6]. In this setting, granulomatous inflammation within the pulmonary parenchyma gives rise to the characteristic atoll appearance on imaging. Patients with paragonimiasis often have a history of ingesting raw or undercooked freshwater crustaceans and typically reside in or have traveled to endemic areas [3, 6]. In addition, laboratory evaluation may reveal peripheral eosinophilia and elevated serum IgE levels, features that are uncommon in bacterial or fungal infections.
Fig. 7
Atoll sign (arrows) in a patient with pulmonary paragonimiasis. Chest CT images with (A) lung window and (B) mediastinal window settings demonstrate a solitary, right lower lobe lateral basilar, subpleural irregular pulmonary opacity with the atoll sign (arrows) and surrounding ground-glass opacity (*). Note the adjacent pleural thickening
Inflammatory and autoimmune diseasesOrganizing pneumoniaOrganizing pneumonia (OP) is the prototypical condition linked to the RHS and often presents with bilateral, peripheral lesions in patients experiencing insidious symptoms such as cough or dyspnea. In OP, the central GGO reflects acute inflammatory and fibrinous exudates filling the alveoli, while the outer rim of consolidation represents organizing fibrosis. OP typically demonstrates a smooth, uniform rim of consolidation and may exhibit a migratory pattern on serial imaging, characteristics that are less common in infectious or neoplastic processes (Fig. 8) [7].
Fig. 8
Examples of the reverse halo (atoll) sign (arrow) in a patient with breast cancer and organizing pneumonia (OP). The images demonstrate the characteristic peripheral and bronchovascular distribution of the pulmonary opacities
Vasculitis and autoimmune disordersAutoimmune disorders such as granulomatosis with polyangiitis (GPA) and systemic lupus erythematosus (SLE) can present with the RHS. In GPA, the central ground-glass opacity reflects necrotizing granulomas or vasculitic lesions, while in SLE, lupus pneumonitis or alveolar hemorrhage produces a similar pattern (Figs. 9 and S3) (1–4). Eosinophilic pneumonia (EP), though rare, is characterized by alveolar inflammation with eosinophilic exudates and a peripheral rim of consolidation, accompanied by peripheral eosinophilia and elevated IgE levels (Fig. 10) [8]. Diagnosis is achieved by correlating imaging findings with clinical clues: for example, GPA often presents with systemic features such as sinusitis or renal involvement with positive ANCA, SLE is typically accompanied by malar rash, arthritis, and positive anti-dsDNA antibodies, and eosinophilic pneumonia usually manifests as upper lobe peripheral RHS lesions with marked eosinophilia.
Fig. 9
Examples of the atoll sign (arrows) in patients with (A, B) granulomatosis with polyangiitis, (C, D) systemic lupus erythematosus, and (E, F) rheumatoid arthritis. The images demonstrate the characteristic reverse halo sign in different autoimmune conditions, highlighting variations in distribution and associated pulmonary changes
Fig. 10
A Coronal and (B) axial chest CT images demonstrate upper lung-predominant ground-glass opacity (GGO) and the reverse halo sign (arrows) in a patient diagnosed with eosinophilic pneumonia. The patient had peripheral eosinophilia of 1264 eosinophils/μL (normal range ≥ 500 eosinophils/μL)
SarcoidosisSarcoidosis, a multisystem granulomatous disease, can sometimes produce coalescent nodules that form a RHS (Figs. 11). In this setting, the central area often represents active granulomatous inflammation, while the surrounding consolidative rim reflects an evolving granulomatous reaction. Radiologists can differentiate sarcoidosis from other causes of the atoll sign by identifying additional imaging features—such as bilateral hilar and mediastinal lymphadenopathy and a characteristic bronchovascular or perilymphatic distribution of nodules—that are typical of sarcoidosis but less common in organizing pneumonia, infections, or malignancies [1,2,3,4, 9]. Clinically, patients with sarcoidosis often exhibit systemic symptoms including fatigue, cough, and sometimes skin or ocular involvement, and may have supportive laboratory findings such as an elevated angiotensin-converting enzyme (ACE) level.
Fig. 11
Reverse halo (atoll) sign (arrows) in two different patients with sarcoidosis. A Axial chest CT image shows multiple tiny coalescing nodules in the right upper lobe forming the atoll sign. B Axial chest CT image of a patient with alveolar sarcoidosis demonstrates left upper lobe consolidation with central ground-glass opacities consistent with the atoll sign
Lipoid pneumoniaLipoid pneumonia results from the aspiration or inhalation of lipid-containing material, leading to the accumulation of lipid-laden macrophages within the alveolar spaces. In some cases, these lipid deposits produce a RHS on CT imaging [1, 2]. Patients with lipoid pneumonia often have a history of chronic aspiration, neurological deficits, or occupational exposure to oil-based substances, such as mineral oil or vegetable oil. On CT, lipoid pneumonia may exhibit areas of negative attenuation within the consolidation—reflecting the fat content—a feature that is typically absent in organizing pneumonia or infectious etiologies [1, 2]. Additionally, these patients usually lack systemic signs of infection.
Vascular causesPulmonary Embolism (PE)PE can lead to wedge-shaped infarcts that manifest as the RHS, typically in the posterior or basal segments of the lung (Fig. 12). The central GGO represents ischemic lung parenchyma, and the surrounding consolidation reflects inflammatory hemorrhage or partial necrosis [3]. Clinically, patients with PE often present with acute onset dyspnea, pleuritic chest pain, and sometimes signs of right heart strain, and they usually have predisposing conditions such as deep vein thrombosis or hypercoagulable states. The PE-related RHS is characteristically wedge-shaped and peripherally distributed. Elevated D-dimer levels and findings on CT pulmonary angiography, such as direct visualization of intraluminal thrombus, further support the diagnosis [3, 4].
Fig. 12
Atoll sign in a patient with pulmonary embolism. The patient had been monitored as an inpatient due to arrhythmia and developed chest pain over the past 24 h. A The frontal radiograph shows a peripheral, wedge-shaped opacity in the right mid-lung (white arrow). B Sagittal and (C, D) axial chest CT angiography images demonstrate pulmonary embolism (orange arrows) and a right lower lobe posterior basilar wedge-shaped pulmonary opacity with the atoll sign (red arrows), consistent with pulmonary infarction
Septic pulmonary embolismIn septic pulmonary embolism the RHS may indicate infected infarcts (Fig. 13). These lesions are typically characterized by cavitation and the presence of multiple peripheral nodular opacities, which suggest an embolic process [1,2,3,4]. Unlike the smoother, more uniform appearance of OP or the solitary nature of certain neoplastic lesions, septic emboli often exhibit a heterogeneous and irregular morphology. Clinically, these patients usually present with signs of systemic infection, such as fever, elevated inflammatory markers, and positive blood cultures, as well as established risk factors like IV drug use or a history of endocarditis [3, 4].
Fig. 13
Atoll sign (arrows) in a patient with colon carcinoma and presented with cough and fever. The patient diagnosed with septic pulmonary embolism due to Bacteroides fragilis septicemia. Axial (A) mediastinal and (B) lung window CT images demonstrate a solitary, right upper lobe anterior wedge-shaped opacity with the atoll sign. Note the surrounding ground-glass opacity (*), indicative of associated inflammation, hemorrhage, or infarction
Malignant causesPrimary lung carcinomaRarely primary lung cancers can exhibit the RHS (Fig. 14). In these malignancies, the central GGO often corresponds to tumor necrosis [10]. Lung cancer–related RHS is typically observed in patients with risk factors such as a significant smoking history, unexplained weight loss, and a more insidious clinical course without the acute infectious symptoms. On CT, malignant lesions may display irregular or spiculated margins, and they are more likely to be associated with adjacent lymphadenopathy or satellite nodules. Furthermore, unlike benign conditions that often improve with appropriate therapy, malignant lesions tend to persist or progress on follow-up imaging [3, 10].
Fig. 14
Reverse halo (atoll) sign (arrows) in two patients with primary lung carcinoma. A, B A patient with lung squamous cell carcinoma: Axial (A) mediastinal and (B) lung window CT images show an irregular, spiculated right upper lobe mass with the atoll sign (arrows). Note the surrounding ground-glass opacity (*), which may reflect an invasive component of the tumor. C, D A patient with invasive pulmonary adenocarcinoma: C Axial and (D) coronal chest CT images demonstrate a right middle lobe mass with the reverse halo sign and internal cystic airspaces (arrows)
Metastatic cancerMetastatic lesions from malignancies can also create a RHS (Fig. 15) [4]. Metastasis-related RHS is often characterized by multiple irregular and heterogeneous lesions. In patients with a known history of cancer, the identification of such a pattern, along with associated findings like mediastinal or hilar lymphadenopathy, should prompt a comprehensive metastatic workup and staging [4, 11].
Fig. 15
Reverse halo (atoll) sign in a patient with metastatic malignant melanoma. A, B Chest CT images demonstrate an irregular right upper lobe mass with the reverse halo (atoll) sign (arrows). Metastasis was confirmed via biopsy. Note the presence of additional pulmonary nodules suggestive of metastasis. The patient also had multiple hepatic metastases (not shown)
Trauma and treatment relatedPulmonary contusionPulmonary contusions resulting from blunt chest trauma can produce a temporary peripheral RHS (Fig. 16). In these cases, the central GGO is due to alveolar hemorrhage and edema, while the peripheral rim of consolidation reflects the organizing inflammatory response to the injury. Pulmonary contusions are typically associated with a clear history of recent trauma and often present with concurrent clinical findings such as chest wall bruising or rib fractures. Moreover, these traumatic lesions characteristically resolve within a few days on follow-up imaging [1, 2].
Fig. 16
Reverse halo (atoll) sign in a patient with blunt chest trauma. Axial chest CT image demonstrates multiple subpleural pulmonary opacities with the atoll sign (arrows), likely reflecting pulmonary contusion. The patient also had non-displaced rib fractures (not shown)
Radiation-Induced Organizing Pneumonia (RIOP)Patients who have undergone thoracic radiotherapy may develop radiation-induced organizing pneumonia (RIOP). In RIOP, the RHS can appear both within and outside the radiation field, reflecting a widespread inflammatory and fibrotic response in susceptible lung segments (Figs. 17 and S4) [1, 4,
Comments (0)