
Remember me
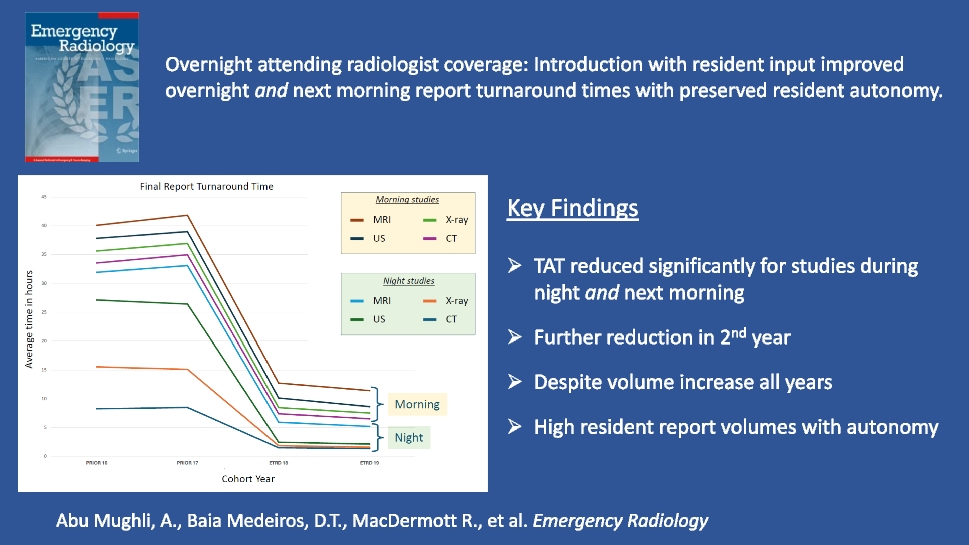
To evaluate the impact of overnight in-house emergency radiologist coverage on turnaround time (TAT) for emergent imaging of ED and inpatients, during the night and following morning, in a coverage model tailored to preserving resident autonomy.
MethodsRetrospective analysis of TAT for all emergent imaging of ED and inpatients at an academic Level-1 trauma center from September 2015 to August 2019, two years before and after changing coverage model. Median and 90th percentile were assessed for overnight (22:00—07:00 h.) and morning (07:00—10:00 h.) emergent imaging TAT for both the ‘First report’ and ‘Final report’. Statistical significance of TAT changes between study years was assessed with quantile regression. Trainee report volumes and their rotation evaluations were assessed.
Results128,433 emergent ED and inpatient imaging studies (82,482 overnight and 45,951 morning) were included; 40,136 CTs, 83,993 X-rays, 2018 US and 2286 MRIs. Imaging volumes increased over time. Except 90th percentile MRI First report TAT, all overnight TAT metrics statistically significantly improved with the new coverage model. For example, ED CT median Final report TAT decreased from 8.45 h to 1.38 h. Morning imaging showed statistically significant reduction for all TATs, except for MRI TATs and 90th percentile US Final report TAT. For example, ED CT median Final report TAT decreased from 1.56 h to 1.19 h. Absolute imaging volume reported by trainees increased by 14% in the 4-year period and weighted average rotation evaluation on a 5-point scale was 3.9 in the post-implementation cohort.
ConclusionIntroduction of a tailored in-house overnight emergency radiologist coverage model can preserve resident autonomy and productivity while achieving statistically significant reduction of emergent imaging report turnaround time for emergent imaging overnight and the following morning. It may help mitigate ED overcrowding while preserving trainee educational experience.
Graphical Abstract
Comments (0)