In this study, we assessed the clinical outcomes of adult hospitalized patients treated with various antibiotics versus carbapenems for infections caused by AmpC-producing Enterobacterales blood isolates. Empirical treatment choices showed a preference for carbapenems in the majority of patients. The fact that most patients who started carbapenem therapy continued with it as definitive therapy illustrates how initial antibiotic choices influence subsequent treatment decisions.
Our study found a comparable burden of comorbidities between patients treated with carbapenems and those receiving noncarbapenem therapy. Chronic kidney disease, diabetes, and cardiovascular disease were prevalent in both groups, with no statistically significant differences observed. However, cancer and liver disease were numerically higher in the noncarbapenem group. These findings suggest that underlying comorbidities may not have been the primary determinant of treatment choice or outcomes and highlight the complexity of managing AmpC-producing Enterobacterales infections in patients with multiple chronic conditions. The high prevalence of diabetes and chronic kidney disease, in particular, underscores the importance of careful antibiotic selection and dosing, given the potential impact of these conditions on drug pharmacokinetics and patient outcomes. Additionally, the presence of immunocompromised states, such as cancer and transplant status, further emphasizes the need for individualized treatment strategies and close monitoring to optimize clinical outcomes.
While carbapenems were the most commonly used definitive therapy, aminoglycosides and ciprofloxacin were also being considered as alternative treatment options. Notably, we found an underutilization of cefepime, both as empirical and definitive therapy, despite supporting evidence for its efficacy when the MIC is ≤ 2 mcg/ml. Hoellinger et al. and Coyne et al. demonstrated that cefepime was as effective as carbapenems in terms of 30-day mortality, treatment toxicity, and infection recurrence, particularly when the MIC was ≤ 1 mg/l and in patients with moderate-to-high risk Enterobacterales bacteremia [14, 15]. However, clinicians may be hesitant to use cefepime owing to concerns over extended spectrum β-lactamase (ESBL) infections, which are prevalent in our population, as well as the risk of resistance emerging at higher MIC levels (≥ 4 mcg/ml) [16,17,18] Additionally, the role of AmpC β-lactamase in resistance mechanisms may further influence prescribing patterns. AmpC enzymes confer resistance to many β-lactams, including cephalosporins, and can contribute to carbapenem resistance when combined with porin loss, limiting the efficacy of alternative therapies in certain cases. [19,20,21] Moreover, the absence of reported MIC values for cefepime may restrict its clinical utilization and informed decision-making in therapy selection. As a result, broader-spectrum antibiotics such as carbapenems are often prioritized to minimize treatment failure. This underutilization of cefepime points to the need for better integration of cefepime in treatment protocols, potentially as part of antimicrobial stewardship strategies that prioritize more judicious use of broad-spectrum antibiotics.
Our results demonstrated that carbapenems were the preferred choice for treating AmpC-producing Enterobacterales infections, aligning with IDSA recommendations for the management of infections caused by AmpC-producing Enterobacterales [2]. E. cloacae emerged as the most common pathogen, followed by S. marcescens. Our results are consistent with prior studies, confirming the prevalence of E. cloacae as the predominant pathogen causing AmpC bacteremia [14, 15]. Line-related infections were identified as the primary source of bacteremia. The findings underscore the importance of infection control measures, including source control procedures, in which a significant proportion of our patients underwent source control procedures.
In terms of the primary outcome, 30-day mortality occurred in 7.5% of the total patients, specifically from the noncarbapenem group. Previous studies comparing carbapenems with noncarbapenem antibiotics have shown no significant difference in terms of all-cause 30-day mortality rate. These findings align with other studies, such as those by Drozdinsky et al. and Tan et al., which reported no significant differences in 30-day mortality between carbapenems and other antibiotics, including third-generation cephalosporins and piperacillin–tazobactam [22, 23].
Our results further suggest that treatment failure was significantly higher in the noncarbapenem group (20%), often necessitating escalation to carbapenem therapy, compared with just 1.6% in the carbapenem group. This underscores the efficacy of carbapenems in managing AmpC-producing Enterobacterales infections. Similar trends have been reported in literature. For example, a study evaluated outcomes in patients treated with piperacillin–tazobactam compared with those treated with cefepime and meropenem for bacteremia due to AmpC β-lactamase-producing Enterobacterales. They found treatment escalation in both groups. Specifically, 14% of patients receiving piperacillin–tazobactam required escalation in their antibacterial agents owing to persistent bacteremia compared with 10% of patients in the cefepime or meropenem group, although this difference was not statistically significant (p = 0.63). Their findings suggest that treatment escalation rates were comparable between the two groups, indicating similar clinical responses to the therapies administered [13]. Similarly, the MERINO-2 trial reported a treatment escalation rate of 11% in the piperacillin–tazobactam group versus 3% in the meropenem group, with a risk difference of 8% (95% CI, − 4% to 19%) [9]. Collectively, these findings indicate that while noncarbapenem therapies may show comparable outcomes in some cases, carbapenems remain a more reliable option, particularly in cases involving treatment failure or persistent bacteremia.
The logistic regression analysis demonstrated lower odds of mortality with carbapenem use as definitive therapy and source control; statistical significance was not reached with source control. Age, on the other hand, was a significant factor, with older patients showing higher odds of death. Our findings are consistent with the general trends observed in the management of AmpC-producing Enterobacterales infections [14, 15].
Our study also examined the role of ID consultations. While the association between ID consultation and carbapenem prescription did not reach statistical significance, a recent study by Tang et al. highlighted the value of ID consultations in reducing mortality risk for bloodstream infections, especially with repeated consultations [24].
Carbapenems remain an effective treatment option for AmpC-producing Enterobacterales bacteremia; however, their use is associated with significant ecological consequences, including the selection of carbapenem-resistant organisms and disruption of the gut microbiota [25]. As antimicrobial resistance continues to escalate, there is increasing interest in alternative therapeutic strategies to mitigate these risks. Emerging approaches such as bacteriophage therapy, antimicrobial peptides, and monoclonal antibody-based therapies have shown promise and warrant further investigation as potential alternative options. [26,27,28].
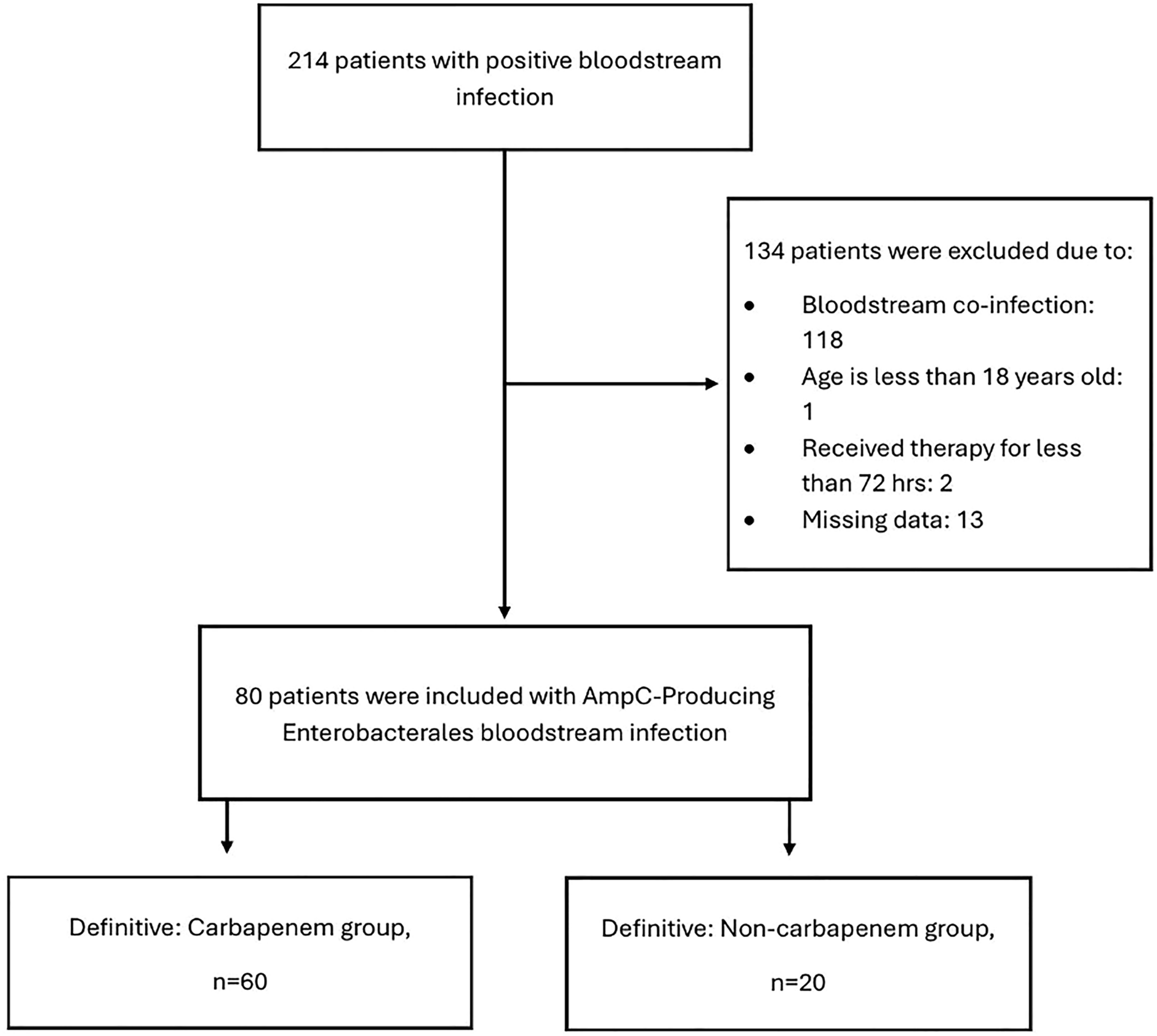
This study has several limitations, including its retrospective observational design, which could introduce the risk of selection bias and difficulty in controlling confounding variables. To mitigate this, we applied strict inclusion and exclusion criteria to ensure a consistent cohort and performed statistical analyses, such as logistic regression, to balance covariates between treatment groups. Additionally, the relatively small sample size could have limited the statistical power to detect differences in outcomes between groups. We reported odds ratios to provide context to the findings, although statistical significance was not reached in some outcomes. However, we acknowledge that larger sample size studies are needed to confirm the findings and to further explore other outcomes. Furthermore, as our study focused on adult patients whose clinical characteristics, antibiotic dosing, and treatment responses differ from those of pediatric populations, future research exploring the effectiveness of carbapenem versus non-carbapenem therapy in pediatric patients would be valuable in addressing this gap.

Comments (0)