
Remember me
A total of 598 publications were identified from the database search (Table S1). After screening for eligibility, 22 publications were included in this review: 19 full-text papers [14, 15, 38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54], 2 PRO development papers [18, 21], and 1 conference abstract [55]. Four blogs/forums were also reviewed and relevant data were extracted (Fig. 2).
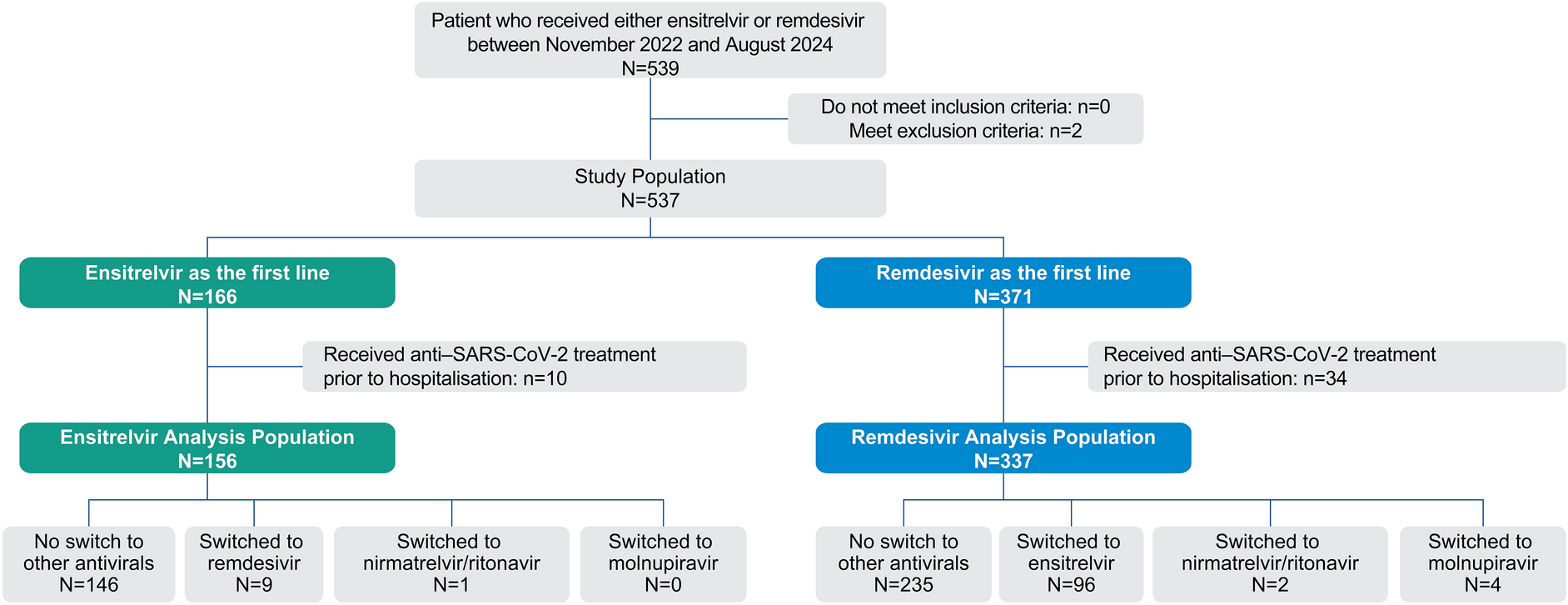
Fig. 2
PRISMA diagram. HSV-2 herpes simplex virus type 2, n number of records, PRISMA Preferred Reporting Items for Systematic reviews and Meta-Analyses, PRO patient-reported outcomes. *The full Google Scholar search returned 11,400 results and only the first 10 pages were screened. The high number of results were due to the limited availability of advanced search filters on the platform, making it less suited for executing a robust and focused search strategy compared to the OvidSP platform
The literature review informed the development of a preliminary conceptual model that was divided into signs/symptoms and HRQoL impact concepts (Figs. S1, S2). A total of 30 signs/symptoms were identified and categorized into six domains: pain, sensory, dermatological, gastrointestinal and urinary, generally unwell, and other. The most frequently reported symptoms were itching (n = 33), sores/lesions (n = 32), blisters (n = 29), and body pain (n = 16). Similarly, a total of 75 HRQoL impact concepts were identified and categorized into 11 domains: sexual, psychological, emotional, social, decision to disclose HSV-2 diagnosis, sleep, cognitive, physical, care, coping strategies, and other. The most frequently reported impacts were concern/worry (n = 34), abstinence from sex (n = 24), and reduced self-esteem (n = 21).
CE InterviewsParticipant Demographic and Clinical CharacteristicsA total of 30 individuals living with HSV-2 GH were recruited for the CE interviews (Table 2); sampling quotas were met or exceeded for most characteristics (Table 3). Many participants were on antiviral treatments at the time of study enrollment (n = 25/30; 83%; CI = 15; ND = 10). Treatments included either episodic (n = 20/25; 80%) or suppressive (n = 5/25; 20%) antivirals (Supplementary File 1).
Table 2 Participant demographic and clinical characteristicsTable 3 Achievement of participant sampling quotasSigns/Symptoms Associated with HSV-2In total, 21 different signs/symptoms were reported and categorized into six domains: pain, sensory, dermatological, genitourinary, systemic, and other. Itching was the most frequently reported symptom (n = 30/30; 100%), followed by sores/lesions/blisters (n = 29/30; 97%), pain (n = 28/30; 93%), tingling (n = 24/30; 80%), burning (n = 21/30; 70%), tiredness (n = 18/30; 60%), aching (n = 18/30; 60%), and flu-like symptoms (n = 17/30; 57%). Sores/lesions/blisters were most frequently reported as the most bothersome (n = 15) (Fig. 3).
Fig. 3
Most bothersome signs/symptoms reported by CE interview participants (N = 30). CE concept elicitation, N total number of individuals, n number of individuals reporting each sign/symptom. Some participants reported more than one sign/symptom. Numbers/percentages represent individuals reporting the sign/symptom out of the total number of participants (N = 30). *Total number of ND (n = 4) and RND (n = 6) participants are shown as a single subgroup.**Total number of CI participants (n = 20)
All individuals reported itching (n = 30/30; 100%; CI = 20; ND = 10), 28 without interviewer prompts. Itching was reported as uncomfortable (6/30; 20%), as a mosquito/bug bite (4/30; 13%), or razor burn/shaving irritation (2/30; 7%). Almost half experienced itching during most episodes of HSV-2 GH (14/30; 47%), mostly in the genital/groin area (22/30; 73%). Itching typically lasted for 2–3 days (13/30; 43%).
Among those who reported experiencing sores/lesions/blisters (n = 29/30; 97%; CI = 19; ND = 10), 28 reported it spontaneously (Fig. 4). Sores (19/29; 66%), lesions (8/29; 28%), and blisters (19/29; 66%) were used interchangeably by some individuals. Just over half experienced sores/lesions/blisters frequently during episodes (16/29; 55%), typically in the genital/groin area (27/29; 93%). The duration of sores/lesions/blisters ranged from a few days (8/29; 28%) to 3 weeks (1/29; 3%), with a majority of episodes lasting for 1–2 weeks (15/29; 52%).
Fig. 4
Participant descriptors of sores/lesions/blisters (n = 29)~. CE concept elicitation, GH genital herpes, HSV-2 herpes simplex virus type 2, N total number of individuals, n number of individuals reporting each descriptor.~Descriptors based on responses reported by ≤ 5 participants are not included in the figure. All quotes presented in the figure are verbatim responses from a participant of a particular subgroup based on the CE interviews. These quotes highlight personal experiences/perspectives of living with HSV-2 GH.*Newly diagnosed (n = 4) and relatively newly diagnosed (n = 6) participants are shown as a single subgroup.**Chronically infected (n = 20)
Almost all individuals experienced pain (n = 28/30; 93%; CI = 20; ND = 8); 23 reported it spontaneously. Most experienced pain from sores/lesions/blisters (24/28; 86%) and over half described their pain as burning (15/28; 54%). Nerve pain (10/28; 36%) was the most frequently reported type of pain unrelated to sores/lesions/blisters. One-third of individuals reported pain at first diagnosis (9/28; 32%). Pain in the genital/groin area was common (10/28; 36%) and lasted 4–7 days (7/28; 25%) in a quarter of the participants.
Over two-thirds of individuals (n = 21/30; 70%; CI = 13; ND = 8) experienced burning, of whom 16 reported it spontaneously. All individuals described a burning sensation (21/21; 100%), with over half finding the burning painful (13/21; 62%). Individuals commonly experienced burning when they were first diagnosed (8/21; 38%), when urinating (7/21; 33%), and in the genital/groin area (9/21; 43%) with burning usually lasting for 1–4 days (7/21; 33%).
Individuals reported experiencing problems urinating (n = 8/30; 27%; CI = 5; ND = 3), with 6 reporting it spontaneously. The most common descriptor was an uncomfortable feeling when urinating (4/8; 50%); other descriptors included urinary frequency (3/8; 38%), difficulty urinating (3/8; 38%), or a ‘split’ urine stream (1/8; 13%). Individuals commonly experienced problems urinating when first diagnosed (3/8; 38%) with a duration of 7–10 days (4/8; 50%).
HRQoL Impact of HSV-2 GH InfectionOverall, 37 impact concepts were identified from the CE interviews and categorized into nine domains related to the impact of HSV-2 GH on HRQoL. These included: psychological/emotional (n = 30/30; 100%), sexual (n = 29/30; 97%), social (n = 25/30; 83%), activities of daily living (ADL) (n = 24/30; 80%), medical support (n = 22/30; 73%), physical (n = 15/30; 50%), work (n = 11/30; 37%), sleep (n = 8/30; 27%), and cognitive (n = 6/30; 20%) (Fig. 5).
Fig. 5
Impact of recurrent HSV-2 GH on HRQoL~. CE concept elicitation, GH genital herpes, HRQoL health-related quality of life, HSV-2 herpes simplex virus type 2, n number of individuals per group reporting each impact. ~ All quotes presented in this figure are verbatim responses from participants in the CE interviews. These quotes highlight their personal experiences and perspectives on living with HSV-2 GH. *Newly diagnosed (n = 4) and relatively newly diagnosed (n = 6) participants are shown as a single subgroup. **Chronically infected (n = 20).±Total number of participants who responded to questions related to the specific QoL impact
All individuals reported psychological/emotional impacts on HRQoL (n = 30/30; 100%; CI = 20; ND = 10). Anxiety and worry (30/30; 100%; CI = 20; ND = 10), loss of self-esteem/confidence (25/30; 83%; CI = 19; ND = 6), and depression and low mood (24/30; 80%; CI = 18; ND = 6) were most frequently reported. Some individuals reported that their diagnosis caused them to feel anger (9/30; 30%; CI = 5; ND = 4), and the diagnosis generally had a negative impact on their mental health (6/30; 20%; CI = 6). Only three participants (10%; CI = 2; ND = 1) noted that they had come to terms with their HSV-2 GH diagnosis, while two (7%; CI = 2) reported feeling guilty for not being careful or safe when having ‘casual’ sex, as they believed that to be the cause of their infection.
Most individuals reported that their sexual relationships were impacted by HSV-2 GH (n = 29/30; 97%; CI = 19; ND = 10). This included abstinence from sex (17/29; 59%; CI = 10; ND = 7) and using condoms to avoid transmission (16/29; 55%; CI = 9; ND = 7). Several individuals reported avoiding ‘casual’ sex (8/29; 28%; CI = 7; ND = 1) and a lack of enjoyment of sex (7/29; 24%; CI = 5; ND = 2). Some reported a negative attitude toward sex (4/29; 14%; CI = 2; ND = 2), that they felt a strain on their current sexual relationships (3/29; 10%; CI = 1; ND = 2), that they would purposely delay sex with a new partner (3/29; 10%; CI = 2; ND = 1), that they felt a low level of intimacy (2/29; 7%; CI = 2), and that they were less likely to masturbate (2/29; 7%; CI = 2).
Social relationships were also impacted (n = 25/30; 83%; CI = 18; ND = 7) with individuals showing concerns about disclosing diagnosis (23/25; 92%; CI = 18; ND = 5), dating concerns (18/25; 72%; CI = 13; ND = 5), feelings of stigma (16/25; 64%; CI = 12; ND = 4), feeling a strain on romantic relationships (15/25; 60%; CI = 13; ND = 2), finding it difficult to attend social events (12/25; 48%; CI = 8; ND = 4), and fear of rejection (11/25; 44%; CI = 7; ND = 4). Individuals reported that infection made them feel lonely (9/25; 36%; CI = 5; ND = 4), or less likely to have a baby due to worries about GH impacting either the baby’s health or their own (7/25; 28%; CI = 3; ND = 4), and felt that their non-romantic relationships (e.g., with friends and family) were strained (7/25; 28%; CI = 6; ND = 1).
Most individuals reported that their daily activities were impacted by GH (n = 24/30; 80%; CI = 17; ND = 7). The most commonly reported impact on daily activities was avoidance of wearing certain types of clothing (18/24; 75%; CI = 13; ND = 5) that would exacerbate or trigger their signs/symptoms.
Most individuals reported experiencing a lack of medical support in relation to HSV-2 GH (n = 22/30; 73%; CI = 14; ND = 8). These participants reported a lack of information and communication from healthcare providers when first diagnosed (n = 17), and difficulties faced during admission/testing as providers were reluctant to test for HSV-2 (n = 5).
Concept SaturationSaturation analysis for spontaneously reported sign/symptom and impact concepts was conducted for the CI participants (n = 20) as this was the population of interest for this study. Over half of the sign/symptoms (n = 12/21; 57%) were spontaneously reported in the first two groups of interviews, and five signs/symptoms (n = 5/21; 24%) were spontaneously reported for the first time in the third group of interviews. No new concepts emerged in the fourth/last group of interviews and saturation was deemed to be achieved (Tables S4, S5).
Final Conceptual ModelThe final conceptual model was informed by the preliminary conceptual model, CE interviews, and expert clinician guidance. After including only recurrent episodes of HSV-2 GH, data from 26/30 individuals contributed to the model.
The final model (Fig. 6) included 35 signs/symptoms categorized into six domains: pain, sensory, dermatological, genitourinary, systemic, and other. Additionally, 59 HRQoL impacts were identified and organized into nine domains: sexual, psychological/emotional, social, sleep, cognitive, physical, work, medical support, and other.
Fig. 6
Conceptual disease model of HSV-2 GH infection*. a Signs/symptoms and b Impact on HRQoL. CE concept elicitation, GH genital herpes, HRQoL health-related quality of life, HSV-2 herpes simplex virus type 2, n number of records included in the literature review and number of individuals in the interviews, PRO patient-reported outcomes.*Frequency counts indicate how often each concept was reported. For the peer-reviewed papers found through the OvidSP search and the PRO developmental papers, the number of individuals who experienced each concept was not reported. Thus, the “n” numbers for these concepts refer to the number of papers mentioning the concept, not the number of individuals. For the blogs/forums and conference posters, participant numbers were provided, so the “n” values represent individual reports
Most signs/symptoms and HRQoL impact concepts were reported in both the literature review and CE interviews. Notably, two signs/symptoms [dermatological (n = 1/35) and systemic (n = 1/35)] and five impact concepts [psychological/emotional (n = 1/59), social (n = 3/59) and sexual relationships (n = 1/59)] were unique to the literature review. Those unique to the CE interviews included four signs/symptoms [dermatological (n = 1/35), pain (n = 2/35) and genitourinary (n = 1/35)] and 12 impact concepts [social (n = 2/59), sexual (n = 3/59), ADL (n = 3/59), work (n = 2/59), sleep (n = 1/59), and cognitive (n = 1/59)].
When considering CI and ND individuals, only two impact concepts [sexual (n = 1/59) and ADL (n = 1/59)] were reported exclusively by the CI individuals.
Conceptual MappingThe signs and symptoms from the final conceptual model were mapped onto the HSC items, while impact concepts were mapped to the HOIQ and RGHQoL items to assess the coverage of these PRO measures (Fig. 7). The HSC covered most identified domains (5/6; 83%), including sensory, pain, genitourinary, systemic, and other domains. It assessed most sensory signs/symptoms (3/4; 75%), such as itching, tingling and burning, and fully covered pain and genitourinary domains (2/2; 100%). However, it only covered a third of the systemic domain concepts (3/9; 33%) and one concept from the ‘other’ domain (1/2; 50%), specifically bowel movement problems. The HSC did not assess any of the dermatological sign/symptom concepts.
Fig. 7
Conceptual mapping of signs/symptoms and impact concepts onto PRO measures. HQIQ Herpes Outbreak Impact Questionnaire, HSC Herpes Symptoms Checklist, HSV-2 herpes simplex virus type 2, PRO patient-reported outcome, RGHQoL Recurrent Genital Herpes Quality of Life questionnaire
The HOIQ assessed just over half of the identified HRQoL impact domains (5/9; 56%): social relationships, sexual relationships, ADL, work, and physical functioning. The HOIQ addressed various impacts on social relationships, such as strain on romantic relationships and difficulty attending social events. It included one broad item on the impact of HSV-2 on sexual relationships and covered half of the ADL impacts (2/4; 50%) and all physical impacts (3/3; 100%). For the work domain, it captured the difficulty working impact (1/3; 33%). However, it did not assess the psychological/emotional, medical support, sleep, or cognitive domains.
The RGHQoL assessed half of the psychological/emotional concepts (4/8; 50%), including anxiety, mental health, loss of self-esteem, and depression. It covered social relationship impacts (4/13; 31%), such as strain on relationships, disclosing diagnosis, and rejection. Stigmatization was indirectly assessed through items like “worry about people finding out I have herpes.” The RGHQoL broadly assessed sexual relationship impacts (7/9; 78%) and included an item on the difficulty of living with GH covering various daily living impacts. However, it did not assess physical functioning, work, medical support, sleep, or cognition impacts.
Comments (0)