This observational study was conducted as a single-center, chart review, focusing on patients who were prescribed either ensitrelvir or remdesivir for the treatment of COVID-19 in the Rinku General Medical Center, one of four designated medical institutions for specific infectious diseases in Japan. In accordance with the prescribing instruction, ensitrelvir (375/125 mg) was dosed orally once-daily for 5 days, with a 375-mg loading dose on day 1 and 125-mg maintenance doses on days 2–5. Similarly, remdesivir was administered intravenously once daily up to 10 days with a 200-mg loading dose on day 1 and 100-mg maintenance doses from day 2 onwards.
The study was conducted in accordance with the Declaration of Helsinki, and the Ethical Guidelines for Life Sciences and Medical Research Involving Human Subjects. The research protocol was reviewed and approved by the Rinku General Medical Center Clinical Research Ethics Committee (2-23 Rinku Ourai-Kita, Izumisano, Osaka 598-8577, Japan; protocol ID 2024FY-I-003; date of approval 20 August 2024). Patient consent was acquired using an opt-out procedure and no data were included that would allow identification of individual patients.
All hospitalized patients with COVID-19 who received either ensitrelvir or remdesivir between November 2022 and August 2024 were included in the study. Only patients for whom the following data were obtained were included in the study population: start and end dates of ensitrelvir or remdesivir; a positive SARS-CoV-2 test result; clinical outcomes of SARS-CoV-2 infection. Patients were excluded from the study population if they were not treated in accordance with the on-label dosage and administration for ensitrelvir and remdesivir, respectively, or if they refused to participate in the study.
Data were collected using electronic medical records. Pseudonymized information was aggregated and analyzed as anonymized data using an anonymization tool (CoNaxs®, Conax Automomation Sdn. Bhd). The study collected general, treatment, clinical, and virological information from all patients (Supplementary Table 1). Disease severity at the start of ensitrelvir/remdesivir administration was classified by the investigator according to the Japanese guidelines on COVID-19 treatment (Supplementary Table 2) [16]. Virological data collected included SARS-CoV-2 virus test results (antigen chemiluminescent immunoassay, RT-PCR). Quantitative antigen level in nasopharyngeal swabs was assessed using Lumipulse® (Fujirebio, Tokyo, Japan), with a maximum viral antigen level of 5000 pg/mL and a cutoff value of 1.34 pg/mL. It has previously been reported that a cutoff value of 89.73 pg/mL corresponds to a cycle threshold (Ct) value of ≥ 35 by quantitative PCR [17]. When estimating the infectivity of SARS-CoV-2, a Ct value ≥ 35 is often used as a marker for non-infectious viral levels [18]. Therefore, we defined viral clearance as an antigen level of < 89.73 pg/mL.
For the analysis population, patients who met any of the following criteria were excluded, but were included in sensitivity analysis 1: (1) were administered molnupiravir or nirmatrelvir/ritonavir at another hospital on the same day or before being admitted to Rinku General Medical Center; (2) started receiving ensitrelvir at another hospital prior to their admission to Rinku General Medical Center; (3) initiated ensitrelvir treatment at Rinku General Medical Center as an outpatient before subsequent hospital admission; or (4) began remdesivir treatment at another hospital before being admitted to Rinku General Medical Center. A sensitivity analysis was also performed in the patients who did not switch to the other antivirals among the analysis population (sensitivity analysis 2).
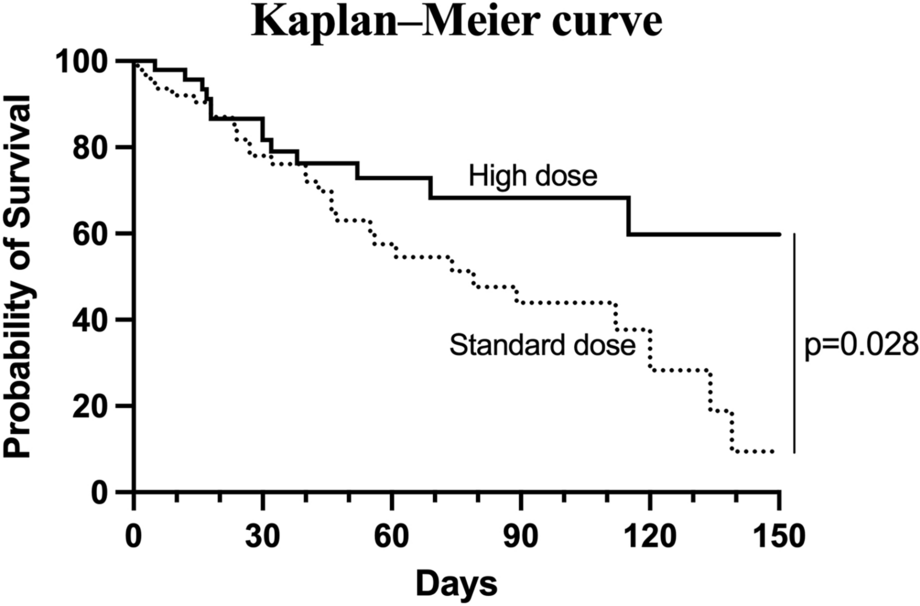
The endpoints of this study included all-cause mortality at day 28, time to discharge, and time to viral clearance up to day 14. For each of these endpoints, estimators were calculated both before and after adjusting for inverse probability of treatment weighting (IPTW). The Kaplan–Meier estimators were used to visually represent and analyze the time to death, discharge, and viral clearance, while hazard ratios for these endpoints between the enstrelvir and remdesivir groups were evaluated using the Cox proportional hazards model. E-values were calculated for the hazard ratio of the outcome to assess the robustness of the conclusions in the presence of potential unmeasured confounding factors [19, 20]. The treatment groups were defined by the treatment that the patient received on day 1 as the first-line treatment.
To standardize the baseline demographic and clinical characteristics across the ensitrelvir and remdesivir groups, propensity scores were computed via logistic regression analysis, and the IPTW method was applied. The covariates used for calculating these scores included age, sex, concomitant diseases (such as diabetes mellitus, dyslipidemia, hypertension, malignant tumors, cardiovascular disease, respiratory disease, liver disease, and kidney disease) considered as the risk factors of aggravation, oxygen demand, COVID-19 severity, dialysis, chemotherapy, immunosuppressant use, SARS-CoV-2 vaccination status, and the presence of pneumonia as evidenced by X-ray. After IPTW adjustment, the standardized mean differences (SMDs) between groups were calculated for each baseline characteristic to check that these were balanced between groups.
Subgroup analyses were carried out on the basis of baseline COVID-19 severity (moderate I, moderate II, or severe patients) [16], immunosuppressive conditions, and vaccination history. An immunosuppressive condition was identified by treating physicians, referring to the Clinical Management Guideline in Immunocompromised Patients by the National Institute of Infectious Disease, as patients with comorbidities such as malignancies and autoimmune diseases or those who received concomitant drugs such as corticosteroids, tacrolimus, methotrexate, and rituximab [21]. No imputation was performed for missing data and no adjustment was made for multiple tests. All statistical analyses were conducted using R software, version 4.1.3.


Comments (0)