
Remember me

Postural responses to GVS have been extensively studied over the years. The primary postural response is a sustained body sway directed toward the anode (Coats 1972). At the start of stimulation, the body leans toward the anodal side, and within 1–2 s, this movement stabilizes, leaving the body in a tilted position. Once the stimulation ceases, all body segments gradually return to their original alignment (Coats 1972; Britton et al. 1993; Day et al. 1997; Séverac Cauquil et al. 2000; Cathers et al. 2005). Consistent responses are observed during walking, with deviations toward the anodal side when subjects walk with closed eyes (Fitzpatrick et al. 1999; Bent et al. 2000; Abbariki 2024). Several researchers have sought to explain the postural response induced by GVS (Fitzpatrick et al. 1994; Hlavacka et al. 1995; Day et al. 1997; Wardman et al. 2003a, b).
One prominent hypothesis, proposed by Fitzpatrick et al. (1994), suggests that the postural response arises from a compensatory effect triggered by an illusion of movement in the opposite direction (toward the cathode). However, studies investigating muscle responses timing have challenged this idea (Britton et al. 1993; Day et al. 1997). These studies highlight two distinct components of the postural response, each with opposite polarities, in response to GVS (Britton et al. 1993). The short-latency component, characterized by its small amplitude and brief duration, occurs approximately 50–60 ms after stimulation onset. Interestingly, its polarity opposes the direction of body sway and is only measured at higher stimulation intensities (Day et al. 1997). In contrast, the medium-latency component has a longer duration, with a latency of around 120 ms, and aligns with the direction of body sway. By contrasting head orientation with respect to gravity, Cathers et al. (2005) showed that short-latency components arise from the otolithic organs while inputs from the SCCs induce the medium-latency response. More recent evidence from Phillips et al. (2013) further supports the canal specific contributions to postural responses. Using localized electrical stimulation of individual semicircular canals, they demonstrated that each canal produces distinct sway directions. These canal-specific responses confirm the differential contributions of otoliths and canal inputs initially highlighted by Cathers et al. 2005. Taken together, these findings support the notion that the sway response to GVS comprises distinct functional components, each associated with specific vestibular inputs. The sway response is indeed actually divided into two different components: a step-like response, hence driven primarily by otolith afferents, and a ramp-like response, driven by canal afferents (Wardman et al. 2003a). The presence of these two components points to the involvement of the vestibulospinal pathway (Baldissera et al. 1990), which operates independently of perceptual processes. Additionally, the difference in their latencies indicates the involvement of distinct central pathways, such as the vestibulospinal and reticulospinal tracts, thought to mediate these responses (Britton et al. 1993; Cathers et al. 2005). Another explanation for the postural response is that its primary function is to maintain the body vertical by minimizing postural muscle activity. This mechanism relies on the integration of vestibular, proprioceptive, and visual inputs to generate a unified estimate of body orientation. GVS disrupts vestibular input, triggering a compensatory realignment of the body to maintain balance (Inglis et al. 1995; Hlavacka et al. 1995). Day et al. (1997) provided a detailed description of these coordinated postural adjustements, involving all body segments: the head tilts relative to the trunk, the trunk shifts over the pelvis, and the pelvis adjusts relative to the ground (Fig. 3). Interestingly, the tilt of the legs is typically about half the magnitude of the tilt observed in the upper body (Wardman et al. 2003b). Day et al. (1997) further proposed that GVS might be interpreted by the body as a tilt of the support surface. This idea is supported by the observation that movements similar to those elicited by GVS naturally occur when the support surface tilts (Purdon Martin 1967). However, findings from Wardman et al. (2003b) suggest differing responses: GVS elicits greater bending when standing on foam, while platform tilt results in more pronounced bending when feet are apart, accompanied by opposite lower body movement (Wardman et al. 2003b). These discrepancies may be explained by rapid sensory reweighting dynamics, as proposed by Assländer and Peterka (2016). Indeed, sensory contributions are not fixed, but rather rapidly rebalanced following sudden changes in available sensory information, affecting postural amplitude, direction, and timing.
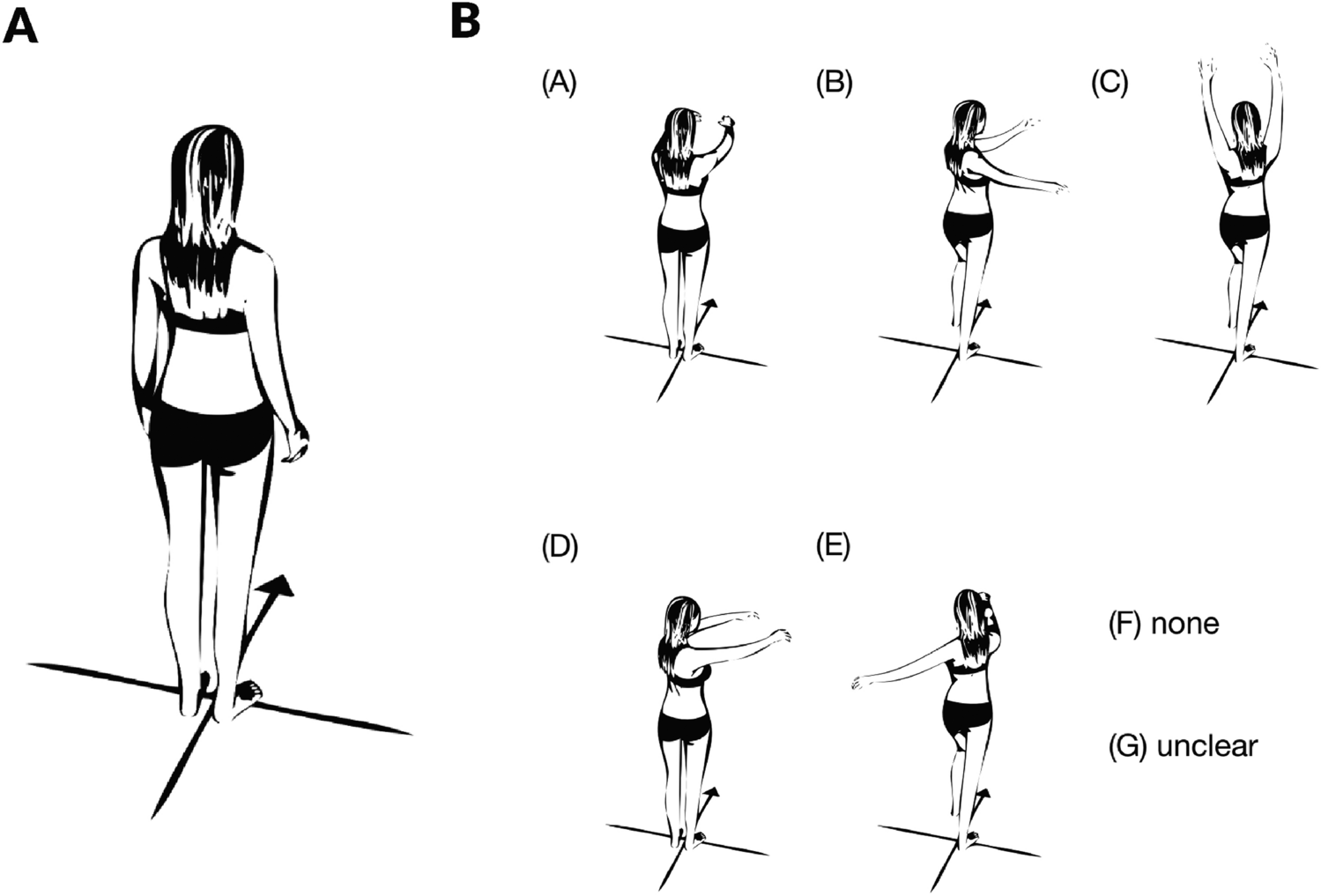
Fig. 3
Typical postural response with sway of the ankles, pelvis, trunk, and head under bipolar binaural GVS (cathode on the right mastoid, anode on the left mastoid), inspired by Day et al. (1997), while the subject looks forward. This response is associated with soleus muscle activity based on Tokita et al. (1989), showing increased activation on the left soleus (red) and decreased activation on the right soleus (blue)
Factors modulating the postural responseHead orientation is a key determinant of sway direction: turning the head to the left shifts the response from a lateral plane to an anteroposterior plane, indicating a head-centered reference frame of the body response (Nashner and Wolfson 1974; Lund and Broberg 1983; Hlavacka and Njiokiktjien 1985; Britton et al. 1993; Pastor et al. 1993; Fitzpatrick and Day 2004).
Balance-engagement of the muscle is essential for generating postural responses. EMG recordings reveal that responses in lower body muscles disappear when the subject is seated but upper body muscles reponse persist if these are involved in maintaining balance (Britton et al. 1993). While seated, the postural response remains present in the trunk and head, though it is less pronounced compared to standing, and the response in the legs vanishes entirely (Day et al. 1997).
Sensory interactions, involving visual and somatosensory inputs, also play a significant role in modulating the postural response to GVS. Deprivation of visual or somatosensory inputs amplifies postural response amplitude (Coats 1972; Britton et al. 1993; Fitzpatrick et al. 1994; Horak and Hlavacka 2001; Day et al. 2010). For instance, postural and muscular responses are amplified when eyes closed and feet positioned close together (Day et al. 1997), and diminished when feet are put apart (Day et al. 1993, 1997). Sensory interactions also influence the shape of response observed: ramp-like responses when there is no sensory interaction, plateau-like responses when visual or somatosensory inputs conflict with vestibular input (Cathers et al. 2005). These conflicting signals modulate the contribution of vestibular input, thereby interrupting the continuous response (Wardman et al. 2003a; Cathers et al. 2005). This type of plateau response has been observed in a subject with impaired sensory afferents, such as in cases of deafferentation, but with significantly greater amplitudes (Day and Cole 2002). Sensory interactions during GVS have also been studied in walking subjects (Fitzpatrick et al. 1999; Bent et al. 2000; Abbariki 2024). Deviation toward the anode is absent with open eyes, highlighting the stabilizing effect of visual inputs (Fitzpatrick et al. 1999). Additionally, slower walking speeds result in greater deviations, reflecting an increased reliance on vestibular input, whereas faster walking relies more on preplanned motor programs, reducing the influence of vestibular and proprioceptive inputs (Fitzpatrick et al. 1999; Bent et al. 2000).
Current intensity modulates both postural and muscular responses to GVS: response amplitudes increase with the intensity (Coats 1972; Petersen et al. 1994; Fitzpatrick et al. 1994), with the largest increase occurring between the torso and pelvis (Day et al. 1997). In walking subjects, deviations toward the anode also increase proportionally with current intensity (Bent et al. 2000). Some studies have identified a linear relationship between current intensity and the displacement amplitude of the center of pressure (Popov et al. 2005). However, this relationship is better described by a power law (exponent 0.55), suggesting a nonlinear transfer between sensory input and motor output (Day et al. 2010). For instance, doubling the stimulus current results in only 73% of the expected response increase. This nonlinearity may provide a functional benefit by amplifying small signals while preventing saturation during larger inputs (Day et al. 2010). These findings appear to align with Forbes et al. (2023), discussed in Sect. «The different GVS configurations » of this review, who reported greater sensitivity and stronger activation of irregular vestibular afferents with increasing current intensity. Although Forbes et al. (2023) did not explicitly quantify a non-linear power-law relationship, their results highlight differential fiber responses consistent with a nonlinear transfer function between current amplitude and neural activation.
Movements induced by brief pulses are restricted to the head relative to the trunk, suggesting the involvement of the medial vestibulospinal tract rather than the lateral one (Fitzpatrick and Day 2004). This goes along with the fact that high frequency movements rarely occur for natural whole-body movement, but rather for head-on-trunk motion. Brief pulses of 2 ms elicit biphasic EMG responses in the ipsilateral sternocleidomastoid and bilaterally in the masseter muscles (Watson and Colebatch 1998; Deriu et al. 2003). These responses primarily involve irregular vestibular afferents, which have lower activation thresholds (Smith and Goldberg 1986), see part 1-anatomy. Sinusoidal stimulation produces frequency-dependent sway, with higher frequencies (> 1 Hz) leading to increased instability, particularly in the lateral direction (Coats 1972; Hlavacka and Njiokiktjien 1985; Petersen et al. 1994). At last, stochastic GVS, has been shown to induce mediolateral sway, primarily within the 1–2 Hz range, while minimizing anteroposterior responses, highlighting the frequency-dependent nature of postural control (Pavlik et al. 1999), but also the directionality of the montage (see part 1). Pink noise enhances vestibular sensitivity at lower intensities (Gavriilidou et al. 2024) likely as a consequence of nGVS increasing the gain and sensitivity of vestibular afferents (Gavriilidou et al. 2024, see part 1). The effects of nGVS on posture is increasingly explored, as highlighted in a recent review that compiles studies investigating its influence on postural control (Xie et al. 2024). This study concludes that nGVS can enhance postural control through the stochastic resonance phenomenon when applied at subthreshold levels, with promising potential for vestibular rehabilitation (see Sect. "Therapeutic GVS: applications to central neurological and peripheral vestibular disorders").
Electrode configurations and postural responseAs seen above, the most commonly used setup is the bilateral bipolar montage, inducing lateral body sway toward the anode (e.g. Britton et al. 1993; Fitzpatrick et al. 1994; Day et al. 1997; Séverac Cauquil et al. 2000; Cathers et al. 2005).
Other studies have investigated unilateral montages (see Sect. 1.3 Fig. 1B; Magnusson et al. 1990; Mihalik 1992), which produce a lateral sway toward the anodal electrode or away from the cathodal electrode, with equal amplitude. Later Séverac Cauquil et al. (1997) investigated anteroposterior and lateral sways evoked by monaural monopolar GVS first successively on a rocking platform then simultaneously on a force platform (Séverac Cauquil et al. 2000). They described an induced oblique, stereotyped body sway with the anteroposterior component comprising a forward or a backward deviation when the cathode or the anode was on the mastoid, respectively. The lateral component was twice as small in the monaural mode. The authors conclude that the classic binaural bipolar GVS could result from the addition of two complementary monaural stimulations (see Sect. 1.3 Fig. 2B, Séverac Cauquil et al. 2000).
This was confirmed using double monaural GVS, applying the same polarization on both mastoids (Fig. 2A) to successfully and consistently orientate the GVS response along the anteroposterior axis (Njiokiktjien and Folkerts 1971; Krizkova and Hlavačka 1994; Séverac Cauquil et al. 1998, 2000; Aoyama et al.
Comments (0)