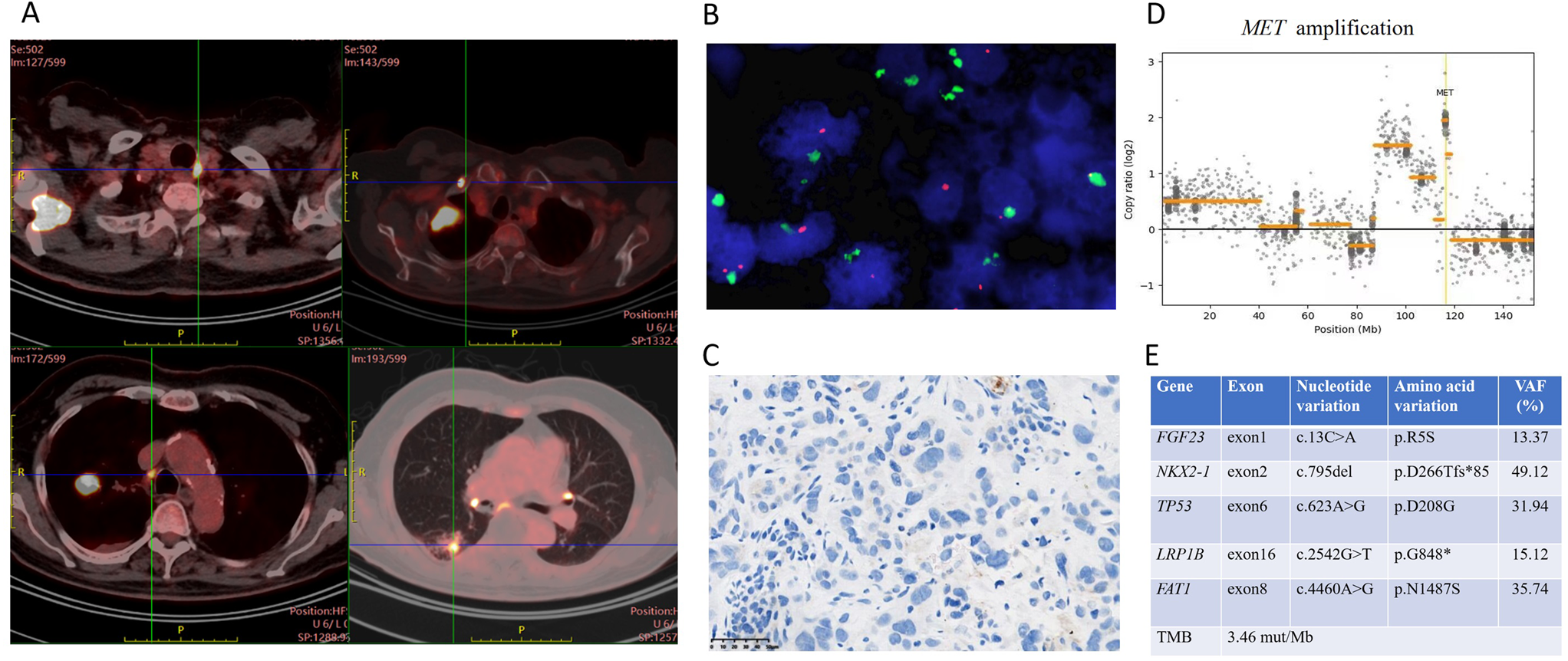
Primary MET amplification is an infrequent oncogenic driver gene variant in lung cancers. Here we report a rare case of advanced lung adenocarcinoma with primary MET amplification in an elderly patient. The individual initially had an ECOG PS 2. NGS analysis of tissue samples demonstrated MET GCN of 8, indicating MET amplification. This finding was confirmed by MET-FISH, which showed cluster amplification. No other oncogenic mutations were detected. PD-L1 TPS was negative. Initial treatment with savolitinib at a dose of 400 mg once daily resulted in a partial response that persisted for more than 16 months. Our report demonstrated the effectiveness and safety of savolitinib as the first-line treatment for advanced NSCLC with primary MET amplification.
MET is known to stimulate cancer cell motility, survival and angiogenesis. (Trusolino et al. 2010) These collectively function as a potent instigator for neoplastic invasion and the development of secondary metastases. Furthermore, it has been observed that certain primary tumors may harbor gain-of-function genetic alterations in the MET gene, which contribute to maintain the transformed phenotype of these tumors.(Trusolino et al. 2010) Increased MET GCN may be caused by focal amplification or polyploidy. (Recondo et al. 2020; Kumaki et al. 2023) Focal amplification refers to an increase in the copy number of a specific gene without simultaneously increasing the copy number of an entire chromosome or a neighboring gene. Polyploidy, on the other hand, is characterized by an increase in copy numbers of an entire chromosome or multiple chromosomes. In the case of MET, polyploidy is typically triggered by a copy number gain on chromosome 7, producing a simultaneous copy number increase in MET and its neighboring genes (e.g., CDK6 and BRAF). (Kumaki et al. 2021)
Presently, numerous TKIs directed towards MET protein have advanced into the clinical setting. Representative clinical trials of MET inhibitors in NSCLC with primary MET amplification are listed in Table 1. It is noteworthy that there are inconsistencies in the inclusion of specific studies and no unanimously agreed upon standards for the identification, classification, and threshold of MET amplification. In studies of crizotinib monotherapy for primary MET-amplified NSCLC, ORR was14.3-38.1% and median PFS was 1.8–6.7 months. Even in the high lever MET-amplification (MET/CEP7 ≥ 4), patients exhibited an ORR of 38.1% and a PFS of merely 6.7 months.(Awad et al. 2016) In another study evaluating the efficacy of crizotinib in patients diagnosed with NSCLC with amplified MET, 15 (78.9%) of the 19 patients analyzed had MET copies of 6 or more based on NGS results. Of these 15 patients, an objective response to crizotinib at a dose of 250 mg orally twice daily was observed in 6 (40%), two of whom also had concomitant MET mutations.(Camidge et al. 2021) Higher levels of MET amplification may correlate with higher rates of tumor response, but this correlation did not lead to a significant improvement in progression-free survival (PFS). Even in the primary treatment population with highly amplified MET (NGS GCN ≥ 10), capmatinib achieved an ORR of 40% and a median PFS of 4.2 months.(Wolf et al. 2020a, b) In addition, tepotinib monotherapy for primary MET-amplified NSCLC showed ORR of 41.7% and median PFS of only 4.2 months.(Xiuning Le et al. 2022a, b).
Table 1 Representative clinical trials of MET inhibitors in NSCLC with primary MET amplificationSavolitinib has recently emerged as a potent MET inhibitor, which has significant in vitro inhibitory activity on MET.(Gu et al. 2019) Based on the results of a pivotal trial in patients with NSCLC/pulmonary sarcomatoid carcinoma, savolitinib was recently granted approval in China for the treatment of metastatic NSCLC with MET exon 14-skipping mutations in patients who have progressed after or who are unable to tolerate platinum-based chemotherapy.(Lu et al. 2021) Although savolitinib in combination with osimertinib has demonstrated inspiring effectiveness in patients with MET amplification following the development of resistance to EGFR-TKI (Hartmaier et al. 2023), data on the efficacy of savolitinib in primary MET-amplified lung cancer are inconclusive. In a retrospective study conducted in China, 34 cases of NSCLC with MET alterations were analyzed. Seventeen patients exhibited MET amplification and six patients were treated with savolitinib. Savolitinib contributed a median PFS of 7.1 months, which was significantly better than the median PFS of 1.4 months observed in patients treated with crizotinib (p = 0.05). (Miao et al. 2023) It is noteworthy that participants in the study with MET amplification had co-existing EGFR-sensitive mutations, and no patients with primary MET amplification were included.
Currently, there is no universal standard or threshold for the detection of MET amplification.(Kumaki et al. 2023) This could potentially result in variable results in different studies. Besides, it should be noted that while MET GCN values can be continuously evaluated and quantified, the specific criteria for positivity may differ. While there was agreement between the MET-to-CEP7 ratio determined by FISH and MET GCN as identified through NGS, this concurrence was not definitive.(Camidge et al. 2021; Peng et al. 2021) Based on the research involving biomarker analysis, MET GCN ≥ 5 determined through NGS was unable to predict a favorable response to MET-TKI therapy.(Peng et al. 2021) In this context, it is critical to consider the possible co-occurrence of oncogenic mutations with the induction of another oncogenic driver pathway. When acquired MET amplification coincides with the activation of driver genes such as EGFR mutations, a single MET-TKI approach is unlikely to provide effective disease control, while combination strategies may be necessary.(Sequist et al. 2020) In this particular case, the individual was elderly and presented with a weakened baseline physical condition alongside advanced lung adenocarcinoma with numerous metastases. MET amplification was detected along with five non-druggable co-mutated alterations (FGF23, NKX2-1, TP53, LRP1B, and FAT1). However, no corresponding targeted therapeutic drugs have been developed for these five co-mutated genes, and these co-mutations may reduce MET-TKI’s effectiveness. Despite these challenging circumstances, the patient experienced an unexpected partial remission that persisted for more than sixteen months following first-line treatment with savolitinib. On the one hand, this can be attributed to the successful suppression of MET activity. Meanwhile, detection of MET amplification via NGS and orthogonal MET-FISH, coupled with the absence of other oncogenic driver genes as indicated by comprehensive genomic profiling (CGP) data, provides further validation for savolitinib’s efficacy as a stand-alone treatment option. The optimal strategy for identifying patients with a higher probability of responding to MET-TKIs may involve the use of integrated MET diagnostic methods and other onco-driver genes detection.



Comments (0)