
Remember me


The use of antimetabolite in Graft-versus-Host Disease (GvHD) prophylaxis after bone marrow transplantation (BMT) in children is controversial. Guidelines of the European Society for Blood and Marrow Transplantation (EBMT) published in 2020 [1] (updated in 2024 [2]) enable, in children undergoing matched-related donor (MRD) BMT, the use of calcineurin inhibitor without an antimetabolite. A survey conducted on behalf of the EBMT in 2020 showed that, in MRD BMT, 45% of the pediatric centers used a combination of cyclosporine plus a short course of methotrexate (CSA/MTX), while 47% used CSA alone [3]. A retrospective analysis of 62 children, published in 2015, is one of the most relevant studies supporting the use of cyclosporine alone [4]. The authors compared childrens receiving CSA vs. CSA/MTX. The former showed reduced cumulative incidence (CuI) of relapse (5% vs. 40%), increased 5-year Overall Survival (OS) (84% vs. 42%), whereas rates of acute GvHD (aGvHD) and chronic GvHD (cGvHD) were similar (P = NS). However, patients who received CSA/MTX had been treated significantly earlier than those who received CSA (1984–1997 vs. 1998–2008, respectively). Therefore other factors, such as more effective chemotherapy protocols, may have influenced outcomes, making the comparison between the two groups challenging.
We report on a homogeneous cohort of children, as we enrolled all consecutive patients who underwent MRD BMT at our center from 2013 to 2023. We retrospectively compared outcomes of patients receiving CSA vs. those receiving CSA/MTX. The decision to add MTX to CSA was made, case by case, considering several factors such as disease (malignant vs. non-malignant), risk of relapse, besides age and stem cells source (SCS), since older age and peripheral blood stem cells are associated with higher risk of GvHD [5, 6]. CSA was initially administered at an dose of 3 mg/kg and subsequently adjusted to achieve a target level of 100–200 ng/mL. CSA was discontinued within six months in the absence of GvHD. CuI of relapse, aGvHD or cGvHD were calculated accounting for competing risks (relapse and death). Multivariable analyses were performed by Cox regression. Further details on statistical methods are provided in the supplementary material.
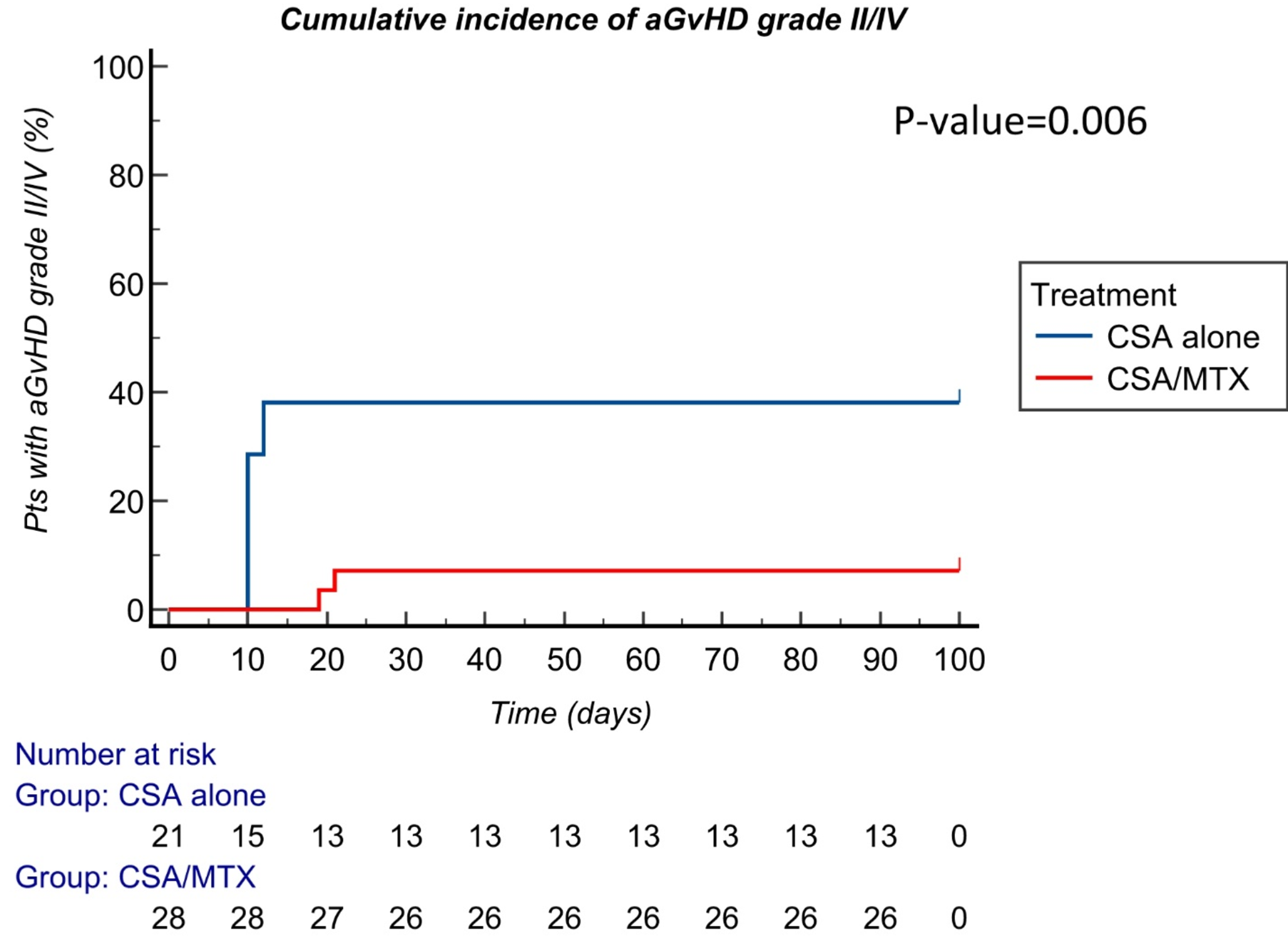
We collected 49 patients. Twenty-one (42.9%) patients received CSA and 28 CSA/MTX (57.1%). Median age was 10.9 years (range, 0.5–21.9). Since the choice of GvHD prophylaxis was influenced by recipients’ age, younger patients (< 12 years old) received more commonly CSA than CSA/MTX (P = 0.0013). Thirty-nine patients (79.6%) had malignancies. SCS was bone marrow in 43 patients (87.5%). Six patients received peripheral blood stem cells: since SCS influences the risk of GvHD, all received CSA/MTX instead of CSA (P = 0.03). Nine patients (18.4%) received antithymocyte globulin (ATG), all of them in combination with CSA/MTX, as previous reports did [7]. Following the publication of Kroger’s study in 2016, ATG was used in 4 patients receiving PBSC as SCS. Five patients with non-malignant disease received ATG, to reduce GvHD, as GvL was not necessary, and promote engraftment. Median follow-up was 4.5 years (range, 0.1–10.1). 5-year OS was 80.7% (95% confidence interval (CI) 62.97-98.44%) in CSA/MTX vs. 83.3% (95%CI 65.96-100.00%) in CSA (P = 0.56). In patients with malignancy, CuI of relapse at 4 years was 33.3% (95%CI 17.2-64.3%) in CSA/MTX vs. 21.36% (95%CI 7.6-60.1%) in CSA (P = 0.27). Overall, 18 patients had aGvHD of any grade (36.7%). CuI of grade II/IV aGvHD at 100 days was lower in CSA/MTX vs. CSA (7.1% [95%CI 1.9-27.1%] vs. 38.1% [95%CI 22.1-65.7%], P = 0.006, respectively) (Fig. 1). When patients who received ATG were excluded from the analysis, CSA/MTX was still associated with a lower CuI of grade II/IV aGvHD than CSA (5.1% vs. 38.1%, P = 0.01) Overall, 16 patients had aGvHD grade I/II (8 had grade I and 8 had grade II). Among the eight patients with aGvHD grade II, 7 received CSA and 1 CSA/MTX: all had skin involvement and one, who was in CSA alone group, had hepatic GvHD. Two patients experienced grade III/IV aGvHD, one in each group. In multivariate analysis only the use of CSA/MTX led to lower incidence of aGvHD grade II/IV (HR 0.1, 95%CI 0.01–0.95, P = 0.04). Overall, 10 patients had cGvHD (20.4%). Three had limited cGvHD only. Skin and liver were the most affected organ (5 patients in each group). CuI of moderate/severe cGvHD at 4 years was 11.9% (95%CI 4.09-34.5%) in CSA/MTX vs. 22.3% (95%CI 9.30- 53.49%) in CSA (P = 0.38). Only use of bone marrow as SCS was associated with lower incidence of cGvHD by multivariate analysis (HR 0.02, 95%CI 0.002–0.243, P = 0.002).
Our study analyzes an homogeneous cohort of patients to prevent potential bias as in previous reports. In patients with malignancy, we did not find an increased risk of relapse using CSA/MTX (P = 0.27). Moreover, CSA/MTX reduced aGvHD, even in a population that received mostly bone marrow as SCS (87.5%). This is of utmost importance since many recent protocols and guidelines (e.g. FORUM study [8] and Italian Group (GITMO) recommendations [9]), enable the use of CSA alone when SCS is bone marrow. Furthermore, in our population, patients receiving CSA/MTX were at higher risk of developing aGvHD since they were older and more often received peripheral blood stem cells vs. CSA alone group (21.4% vs. 0%) [6]. Our study is a retrospective, single-center analysis with a small number of patients, which affects the power of our model, and the majority of whom were younger than 12 years. Despite these limits, we hypothesize that CSA/MTX, compared to CSA alone, may reduce the incidence of aGvHD in children undergoing MRD BMT, while not affecting OS or relapse, thus providing additional, albeit limited, evidence. This combination warrants further investigations in larger, multicentre pediatric studies.
Fig. 1
Cumulative incidence of aGvHD grade II/IV in all patients. CSA: Cyclosporine; CSA/MTX: Cyclosporine plus methotrexate; aGvHD II/IV: acute Graft-versus-Host disease grade II/IV.
Comments (0)