
Remember me


In this study, a cohort of 10,820 patients diagnosed with malignant tumors was enrolled, consisting of 6724 male and 4096 female participants, covering malignancies of the colorectal, gastric, pancreatic, esophageal, biliary tract, and pulmonary systems, among others. KRAS mutations were identified in 2161 out of the 10,820 tumor samples analyzed (19.97%). The prevalence of KRAS mutations exhibited variability among different cancer types, with the highest frequency observed in tumors of the digestive system (1477 out of 4255 cases, 34.71%), followed by tumors of the female reproductive system (146 out of 982 cases, 14.87%). Furthermore, the frequency of KRAS mutations was 11.24% (481 out of 4278 cases) in respiratory tumors, 10.99% (20 out of 182 cases) in soft tissue tumors, and 7.87% (7 out of 89 cases) in bone tumors. In urological tumors, the frequency was 4.19% (9 out of 215 cases), while it was 4.04% (4 out of 99 cases) in neurological tumors, 2.57% (17 out of 662 cases) in head and neck tumors, and 0% (0 out of 58 cases) in breast cancer. The prevalence of KRAS mutations varies among different tumor types, with the highest incidence observed in pancreatic cancer (73.51%), followed by colorectal cancer (41.45%), uterine cancer (21.23%), biliary tract cancer (14.56%), lung cancer (11.24%), gastric cancer (8.57%), thyroid cancer (7.41%), ovarian cancer (5.43%) (Table 1).
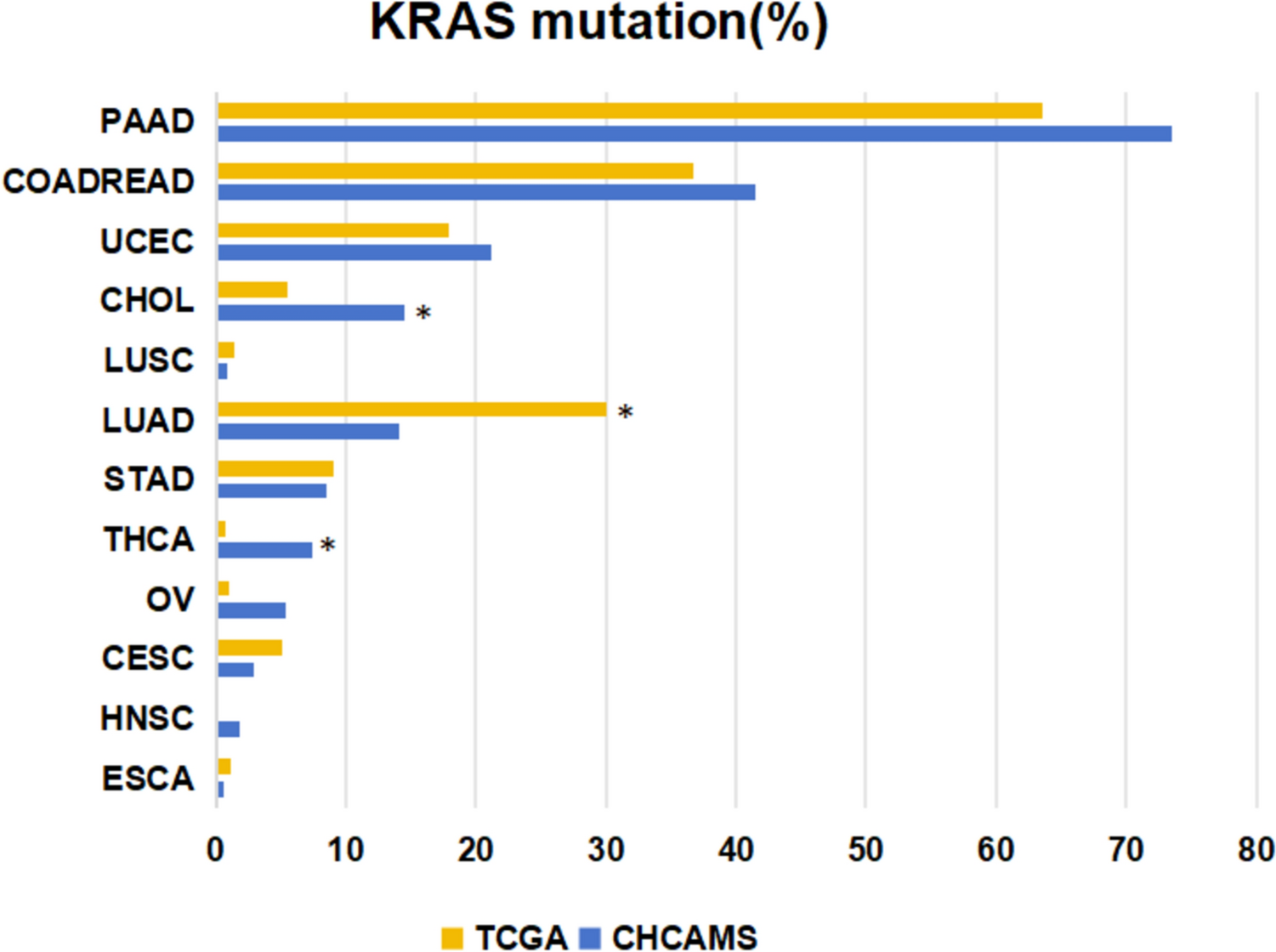
Table 1 The distribution of KRAS mutations across different systems within the studied sample populationFor analytical purposes, only those cancer types that had been observed in more than 50 cases with a KRAS mutation were considered. And then, this epidemiological distribution was compared with data from the TCGA database. The incidence of KRAS mutations was found to be higher in the Chinese NCCN patient cohort compared to the general TCGA population for PAAD (73.51% vs. 63.59%, p = 0.126), COADREAD (41.45% vs. 36.70%, p = 0.562), UCEC (21.23% vs. 17.62%, p = 0.592), and CHOL (14.56% vs. 17.62%, p = 0.038). Conversely, the incidence was lower in patients with LUAD (14.10% vs. 30.05%, p = 0.000) (Figure 1).
Fig. 1
The frequencies of KRAS were different between current data and TCGA in diverse cancers. *p < 0.05
KRAS subtypes in diverse cancersIn pancreatic cancer and colorectal cancer, the G12D mutation was the most common, found in 34.23% and 13.37% of cases, respectively. Uterine cancer predominantly exhibited the G12D and G12V mutations, each accounting for 6.30% of cancer. In contrast, the G12C mutation was most frequently observed in lung cancer, representing 3.37% of cancer. Gastric cancer primarily exhibited the G12D mutation (2.86%) (Fig. 2A). An analysis of KRAS mutations subtypes reveals that the KRAS G12D mutation is the most prevalent in pancreatic, colorectal, and gastric cancers. In contrast, the KRAS G12V mutation predominates in uterine cancer, while KRAS G12C mutation is the most frequent mutation in lung cancer. Specifically, in pancreatic cancer, the KRAS G12D mutation was identified in 46.5% (115 out of 247) of KRAS mutations, followed by KRAS G12V mutation in 31.6% (78 out of 247), and KRAS G12R mutation in 12.5% (31 out of 247) (Fig. 2B). In colorectal cancer, the distribution of KRAS mutations was as follows: G12D mutation in 32.3% (372 out of 1153), G13D mutation in 18.9% (218 out of 1153), G12V mutation in 17.3% (200 out of 1153), and G12C mutation in 6.5% (75 out of 1153) (Fig. 2C). In uterine cancer, the prevalence of KRAS mutations was as follows: G12V mutation and G12D mutations were each present in 29.7% (38 out of 128 cases), G13D mutation in 14.1% (18 out of 128 cases), and G12A mutation in 7.8% (10 out of 128 cases) (Fig. 2D). In lung cancer, the distribution of KRAS mutations was observed as follows: G12C mutation in 29.9% (144 out of 481 cases), G12D mutation in 22.4% (108 out of 481 cases), G12V mutation in 18.9% (91 out of 481 cases), and G12A mutation in 7.3% (35 out of 481 cases) (Fig. 2E). In gastric cancer, KRAS mutations were identified as G12D mutation in 33.3% (20 out of 60 cases), G13D mutation in 28.3% (17 out of 60 cases), and G12V mutation in 10% (6 out of 60 cases) (Fig. 2F).
Fig. 2
Distribution of KRAS mutations in all tumors and seven subtypes. A Proportional distribution of different mutation subtypes in tumors. Distribution and proportion of KRAS mutation subtypes in pancreatic cancers (B), colorectal cancers (C), uterine cancers (D), lung cancers (E) and gastric cancers (F), respectively
Association of TMB with KRAS mutationsThe TMB values of each tumor were assessed through NGS during the identification of driver gene mutations. A TMB of 10 mutations per megabase (mut/Mb) was categorized as high TMB (TMB-H). TMB values demonstrated variability across different malignancies, with TMB-H being most prevalent in gastric cancer (37%, 22 out of 60 cases), followed by uterine cancer (25%, 32 out of 128 cases), lung cancer (25%, 120 out of 481 cases), colorectal cancer (16%, 186 out of 1153 cases), and pancreatic cancer (2%, 6 out of 247 cases) (Fig. 3). In colorectal cancer, significant associations with TMB were observed for the KRAS G13D (p = 0.016) and KRAS G12V (p = 0.005) mutations. In the context of lung cancer, the KRAS G12C mutation showed a positive correlation with TMB-H, with a p-value of 0.000. In uterine cancer, the KRAS G13D and G12V mutations were found to have a significant impact on TMB. In gastric cancer, the KRAS G13D mutation was found to have a significant impact on TMB, indicated by a p-value of 0.025. Conversely, no statistically significant associations were observed in pancreatic cancer (Table 2).
Fig. 3
Distribution of TMB-H in five tumors with KRAS mutations
Table 2 Association of TMB with KRAS mutationsAssociation of MSI status with KRAS mutationsThe status of microsatellite instability high (MSI-H) varied across different malignancies, with the highest prevalence observed in gastric cancer (30%, 18 out of 60 cases), followed by uterine cancer (16%, 20 out of 128 cases), colorectal cancer (7%, 77 out of 1153 cases), pancreatic cancer (0%, 1 out of 247 cases), and lung cancer (0%, 1 out of 481 cases) (Fig. 4). In colorectal cancer, the KRAS G13D (p = 0.000) and KRAS G12V (p = 0.001) mutations exhibited significant effects on MSI-H. In gastric cancer, the KRAS G13D mutation was found to have a significant impact on MSI, indicated by a p-value of 0.015. In contrast, no statistically significant associations were identified in uterine and gastric cancers (Table 3).
Fig. 4
Distribution of MSI-H in five tumors with KRAS mutations
Table 3 Association of MSI with KRAS mutations
Comments (0)