
Remember me



The infant was a 1-month-old male, born at full term with anthropometrical parameters within the standard range for age: weight 3970 g, 51 cm in crown-heel length, and head circumference of 36 cm. The pregnancy was unremarkable, with normal periodic ultrasound scans, and the delivery was spontaneous and uncomplicated. Maternal vaginal and rectal swabs were negative, and she received intrapartum antibiotic prophylaxis.
Approximately 1 month after birth, the infant presented persistent cough, and aerosol therapy was promptly administered. However, after 3 days, he progressively became drowsy and unresponsive. The parents quickly took him to the hospital, but he was already in cardiopulmonary arrest. Cardiopulmonary resuscitation (CPR) was immediately started: oxygen was given through a bag valve mask, and then, an injection of adrenaline was necessary. Despite all attempts, CPR was stopped after 35 min due to pulseless electrical activity (PEA) and the infant was pronounced dead. Subsequent nasal and pharyngeal swabs revealed positive results for respiratory syncytial virus A (RSV), Haemophilus influenzae, and Staphylococcus aureus.
Autopsy findingsAn autopsy was requested to better understand the cause of death. However, in that period COVID-19 was initially spreading, and the lack of medical resources made it necessary to temporarily store the infant’s body at − 10 °C in the freezer of the morgue. Then, due to the health-related challenges arising from the COVID-19 pandemic, the autopsy was delayed for 21 days. Before the autopsy was performed, the body was thawed at room temperature (20 °C) for 12 h.
External examination showed growth parameters within the normal limits for 1 month of age: weight 4301 g (50th percentile), crown-heel length 55 cm (50th percentile), and head circumference 37 cm (25th percentile) [10]. The face was regular with no dysmorphisms. Grossly, no anomalies were identified.
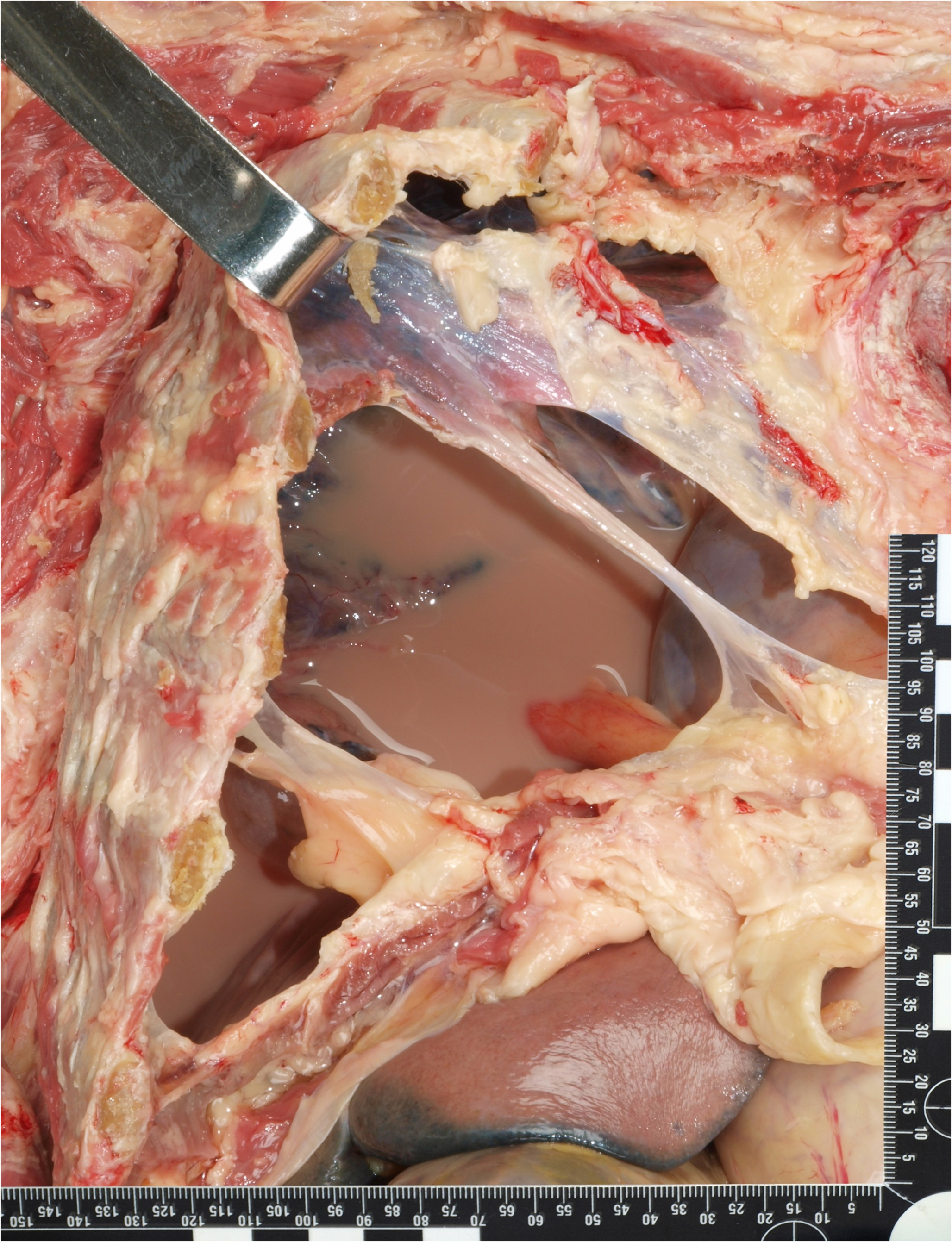
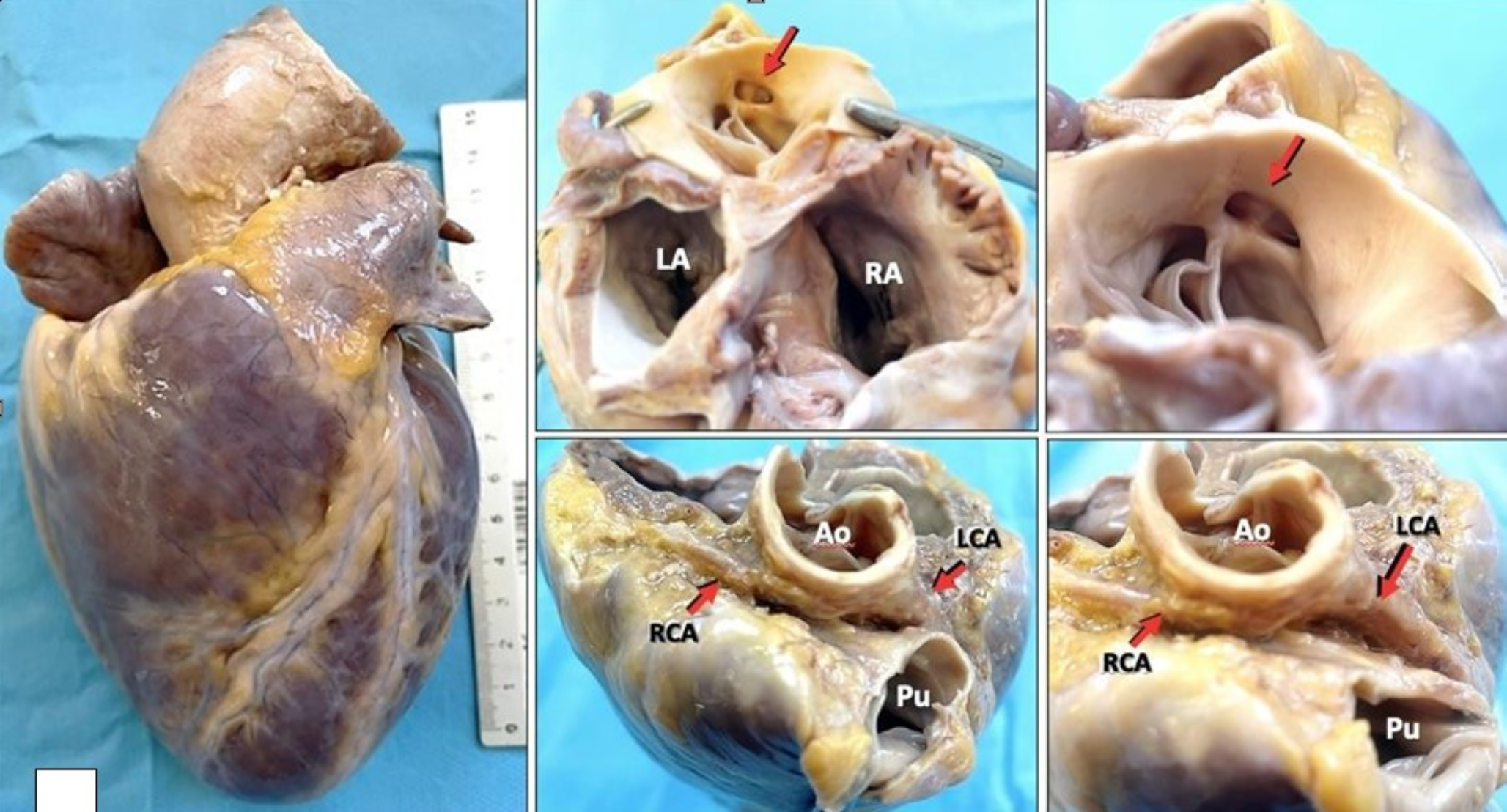
Internal examination evidenced diffuse congestion of the organs, but no anatomical anomalies. The lungs displayed the expected lobes, with three on the right and two on the left. The right lung weighed 61 g and the left 50 g. Segmental sequential analysis of the heart (weight 29 g) revealed atrioventricular and ventriculoarterial concordance and regular systemic and pulmonary venous returns. The coronary arteries presented a regular course. The other organ weights were as follows: liver 173 g, right kidney 20.8 g, left kidney 22.4 g, spleen 16.4 g, brain 489 g.
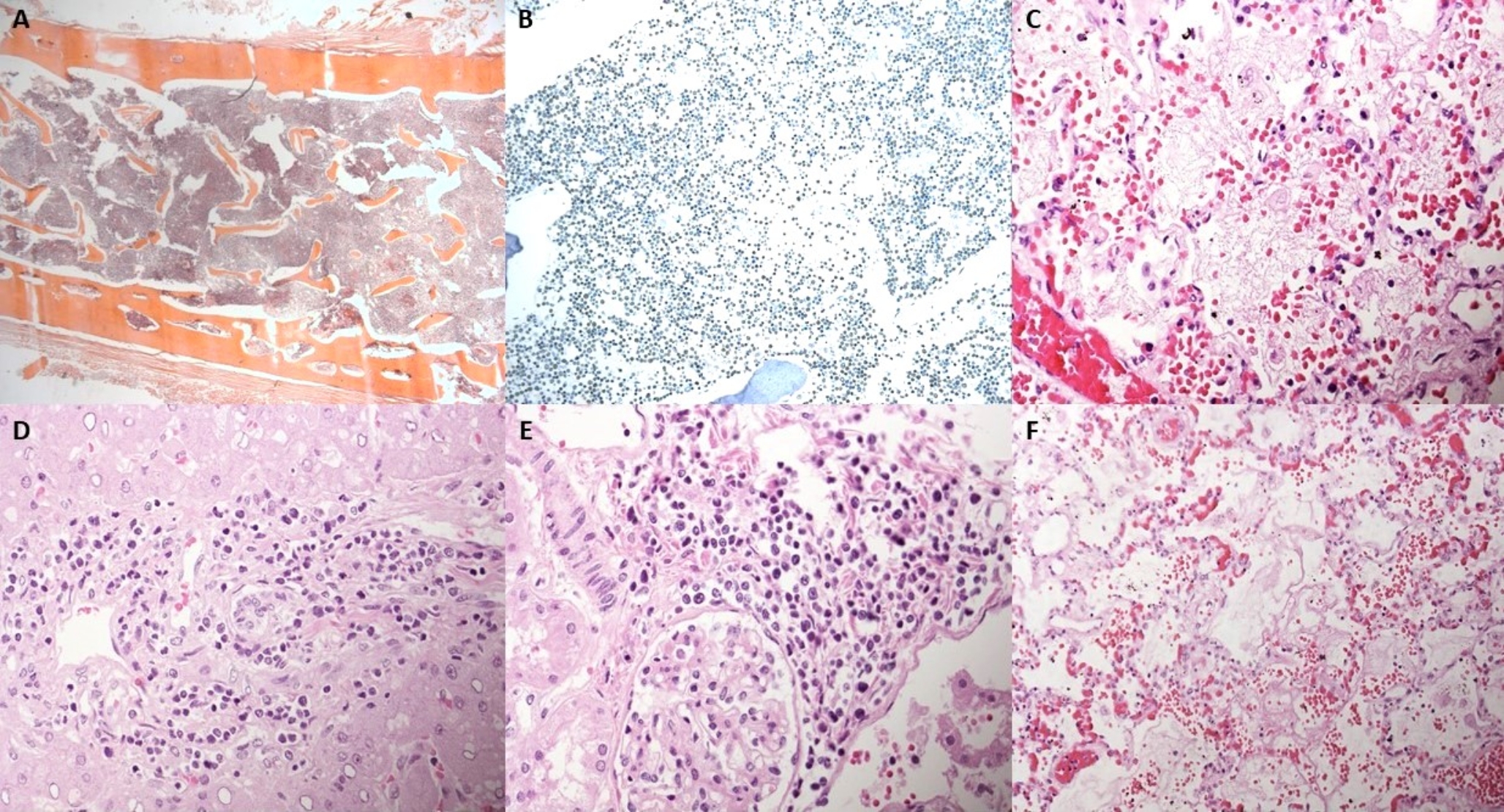
Histological examination of the lungs revealed bilateral extensive acute necrotizing bronchitis and bronchiolitis with focal hyaline membrane formation and pulmonary edema (Fig. 1). Scattered cells with enlarged nuclei due to RSV infection were seen (Fig. 2). Minimal diffuse ischemic changes were observed in the myocardium and brain. Both kidneys showed acute tubular necrosis, tubular dilatation, and occasional microcalcifications. No significant histopathological findings were observed in the other organs.
Fig. 1
Infection of the lungs: diffuse acute necrotizing bronchitis and bronchiolitis together with pulmonary edema (hematoxylin and eosin, 2 HPF)
Fig. 2
RSV infection: a sloughed off cell with enlarged and irregular nucleus compatible with viral inclusion (hematoxylin and eosin, 40 HPF)
The integration of clinical, autopsy, and histological data identified the cause of death as acute respiratory failure resulting from bilateral and diffuse acute necrotizing bronchitis and bronchiolitis. This was caused by RSV type A complicated by bacterial over-infection with Haemophilus influenzae and Staphylococcus aureus.
Histological freeze–thaw artifactsEvidence of histological freeze–thaw artifacts was present in many organs.
The brain disclosed ice crystal artifacts with multiple clefts within the parenchyma (Fig. 3).
Fig. 3
Ice crystal artifacts in the brain: the parenchyma presented multiple clefts compatible with shrinkage of the tissue (hematoxylin and eosin, 10 HPF)
The lungs, apart from histological evidence of infection, exhibited alveolar distension (Fig. 4).
Fig. 4
Freezing and thawing artifacts in the lungs: alveoli were overall distended (arrow); in the same field there was also evidence of bronchiolitis (star) (hematoxylin and eosin, 20 HPF)
The heart presented marked extracellular separation (Fig. 5).
Fig. 5
Heart: marked expansion of the extracellular space (hematoxylin and eosin, 4 HPF)
Abnormal dilatation of lymphatic or capillary vessels was excluded by the regular expression of CD31, which is a marker for endothelial cells, in the vascular structures located between the bundles of cardiomyocytes. Moreover, the artifactual clefts were devoid of endothelial lining (Fig. 6).
Fig. 6
CD31 immunohistochemistry in the heart: the clefts lacked an endothelial cell lining. Small vascular structures were present between the cardiomyocytes (brown staining) (10 HPF)
The liver showed shrinkage of the hepatocellular laminae with marked expansion of the sinusoidal space (Fig. 7).
Fig. 7
Liver freezing and thawing artifacts: A the parenchyma showed shrinkage of the hepatocellular laminae with marked dilatation of the sinusoidal spaces. The aspect seemed to create parallel lines similar to ice crystals (hematoxylin and eosin, 4 HPF); B higher magnification evidenced an unusual hepatic structure resembling hepatic peliosis (hematoxylin and eosin 20HPF); C but immunohistochemical expression of smooth muscle actin (SMA) was not increased (SMA immunohistochemistry, 40 HPF)
The kidneys presented unusual cystic lacunae, probably due to expanded extracellular spaces, with tubules strained and flattened (Fig. 8).
Fig. 8
Kidney artifacts: A the parenchyma presented multiple cystic lacunae, resulting from the expansion of the extracellular spaces, no lacunae were lined by epithelial cells (hematoxylin and eosin, 4 HPF); B some of the tubules appeared stretched and compressed (hematoxylin and eosin, 20HPF)
The thymus structure was almost fully preserved (Fig. 9A). The thyroid presented clefts mostly along the septa, and the cell nuclei appeared more basophilic (Fig. 9B). The acinar architecture of the pancreas was maintained, with a few artifactual lacunae within the septa and the islets were still recognizable (Fig. 9C). On the whole, the cell nuclei appeared shrunk and strongly basophilic. The spleen displayed some cystic slightly eosinophilic spaces devoid of epithelium (Fig. 9D).
Fig. 9
A Thymus: the architecture was overall well maintained with cortex and medullary division (hematoxylin and eosin, 4 HPF). B Thyroid: the only modifications were artifactual clefts along the septa and basophilic cellular changes (hematoxylin and eosin, 4 HPF). C Pancreas: the acinar structure was preserved with few lacunar alterations within the fibrous septa (arrow). The Langerhans’s islets were easily identifiable (star). All the cells were overall more basophilic (hematoxylin and eosin, 4 HPF). D Spleen: a few slightly eosinophilic cystic spaces devoid of an epithelial lining were the only changes observed (hematoxylin and eosin, 4 HPF)
The brown adipose tissue was mainly preserved, but focal cellular shrinkage was seen in the most eosinophilic cells (Fig. 10). The white adipose tissue and the skeletal muscle were virtually unaffected by artifacts (Fig. 11).
Fig. 10
Brown adipose tissue: focal cellular shrinkage was observed in the most eosinophilic cells, the richest in cytoplasmic mitochondria (hematoxylin and eosin, 10 HPF)
Fig. 11
A White adipose tissue (hematoxylin and eosin, 20 HPF) and B skeletal muscle (hematoxylin and eosin, 10 HPF): the overall features were unchanged
Comments (0)