
Remember me



A 59-year-old patient was admitted to the hospital with a diagnosis of lung emphysema Gold IV/D, accompanied by recurrent spontaneous pneumothoraces. Consequently, a left-sided partial lung resection was performed with subsequent intensive care. The postoperative diet was created with EN formula administered via a nasogastric FT. The FT position control was realized by auscultation prior to the administration of EN formula (Nutrison Energy multifibre® tube feed (Nutricia, Germany)) via the FT. The following morning, as part of a routine radiological examination of the thorax, a misplacement of the FT into the right lung was suspected, indicating that EN formula had been administered into the right lung. Accordingly, the tube position was corrected. However, the patient died later that day.
Other specified diagnoses were diabetes mellitus, type II after ethyl toxic pancreatitis and hypertension.
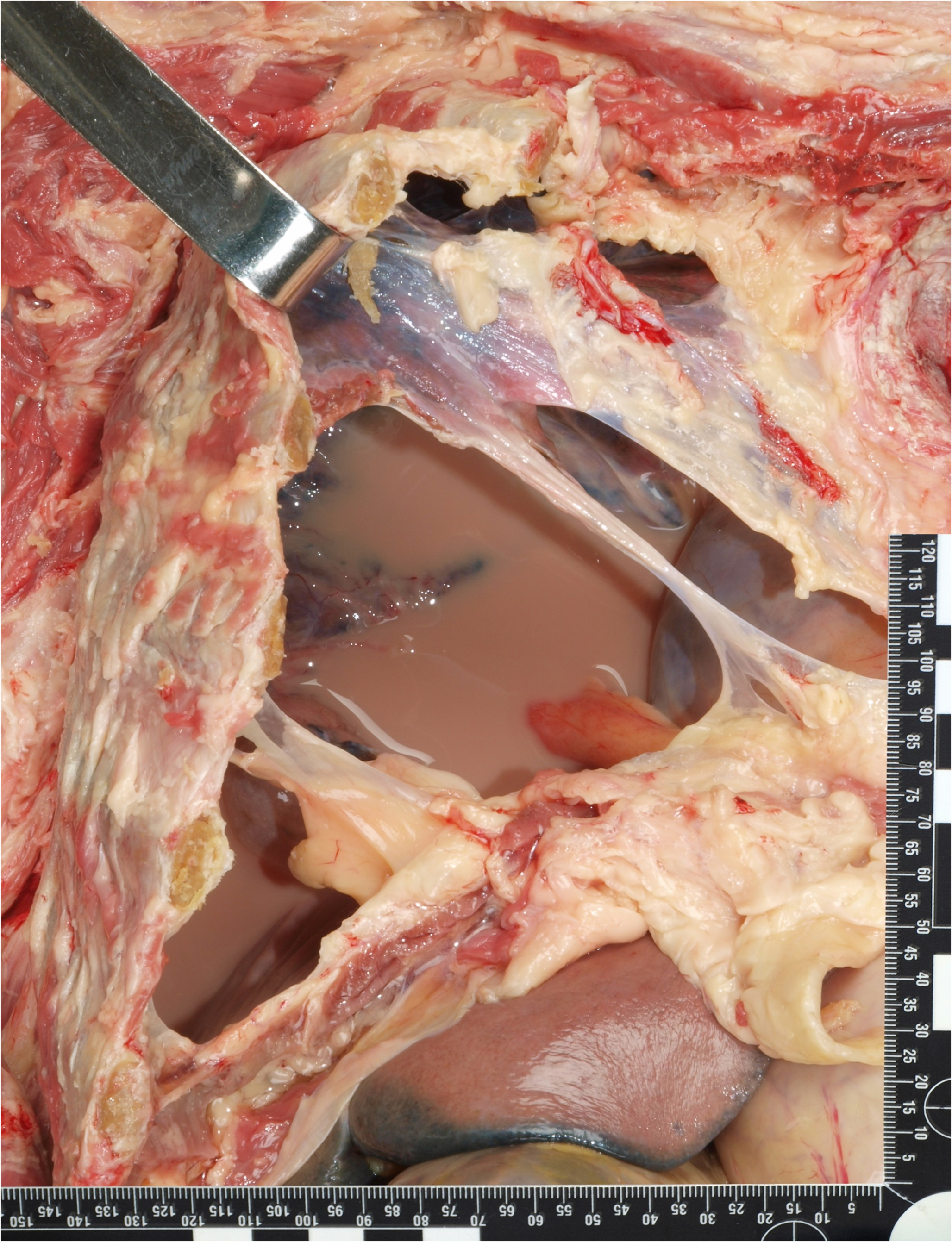
Autopsy and histologyThe aim of the autopsy was to determine whether the leakage of EN formula into the pleural cavity contributed directly to the patient’s death. The autopsy findings revealed bullae consistent with chronic pulmonary emphysema. The surgery was performed without any complications. However, 350 ml of a turbid, milky-brown liquid was detected in the right thFig. (Fig. 1). The airways contained yellowish-brown mucus. In addition, the visceral pleura of the right lung was ruptured in certain areas. The lung tissue displayed a lack of ventilation and was rich in fluids. There was histological evidence of aspiration pneumFig. (Fig. 2). The hypothesis of prolonged oxygen deficiency was substantiated by the histology of the central nervous system, which revealed elective necrosis of nerve cells. Furthermore, corroborative findings included signs of chronic kidney disease, chronic heart insufficiency and coronary disease, as well as signs of the specified arterial hypertension.
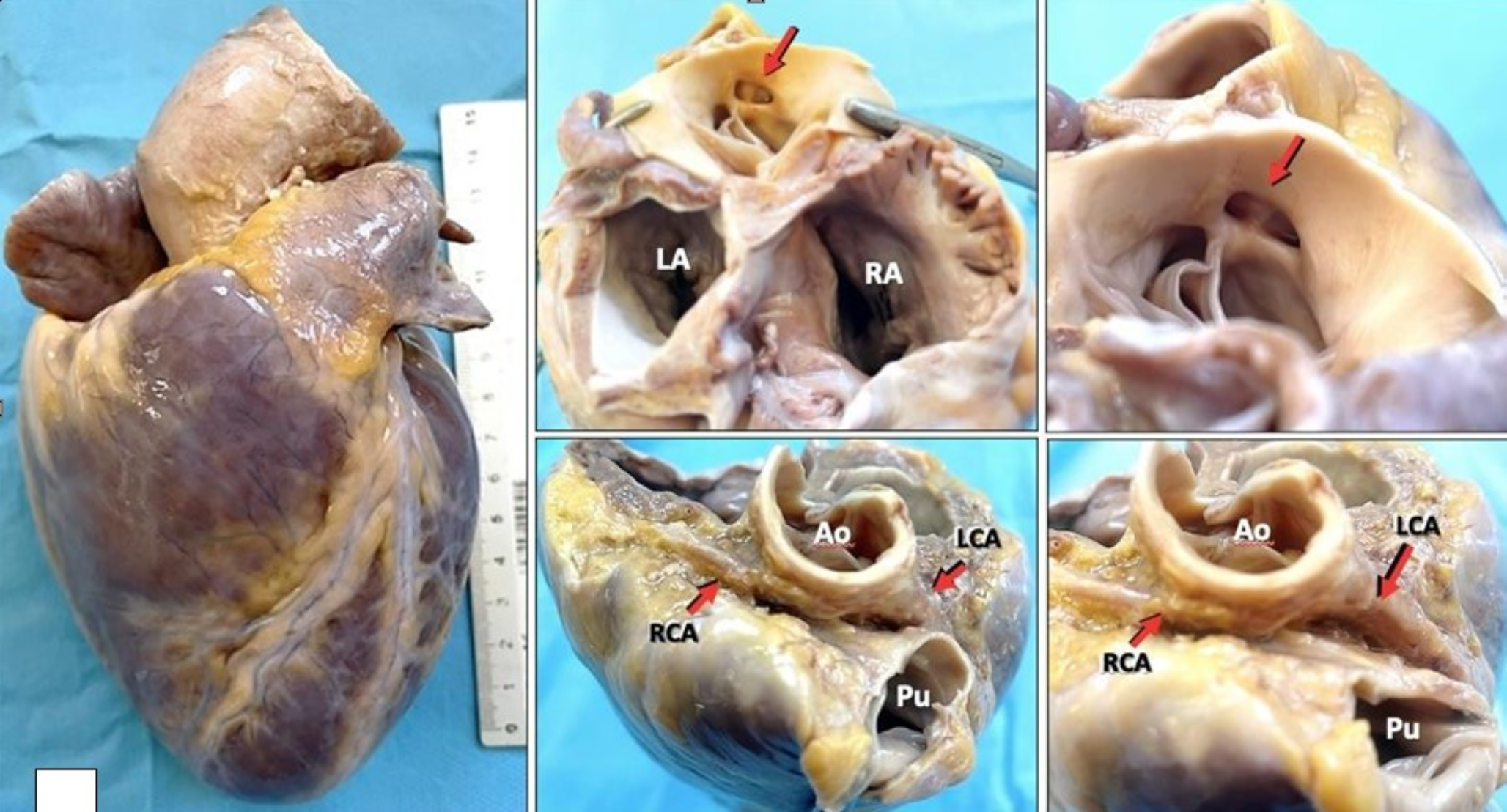
Fig. 1
Autoptic findings of turbid, milky-brown liquid in the right chest cavity
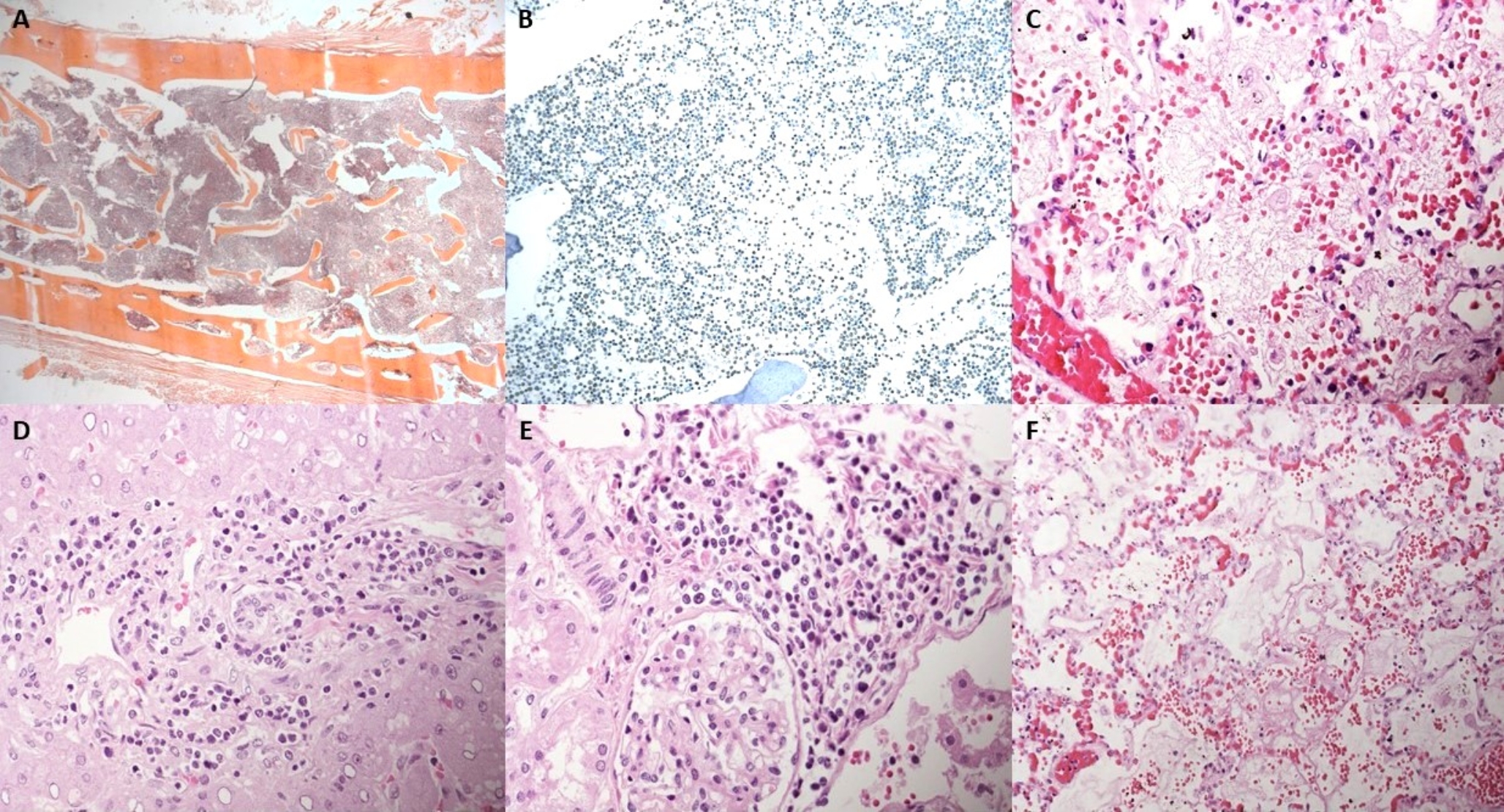
Fig. 2
Histological detection of aspiration pneumonia via hematoxylin‒eosin staining of lung tissue (A) Overview (scale bar 100 μm), (B) closer view (scale bar 25 μm) with a foreign body in polarized light
To elucidate the nature of the liquid in the right thorax, a combination of cytological and chemical-toxicological investigations was performed.
Cytological analysisFor comparison, a specimen of the EN formula Nutrison Energy multifibre® tube feed (Nutricia, Erlangen, Germany) was obtained. Following centrifugation, smears of the EN formula and the pleural effusion from the right thoracic cavity were prepared. The preparations were subsequently stained via different methods, including hematoxylin‒eosin and Congo red (all chemicals were purchased from Carl Roth, Germany).
Numerous granulocytes, predominantly exhibiting a lobed morphology, were found in the right thoracic cavity smear, confirming the diagnosis of pleural empyema. In addition, Congo red-positive material was detected in both the control smear from the EN formula and the pleural effusion smear. The proportions of EN in the chest cavity may be represented by rod-shaped Congo red-positive material (Fig. 3).
Fig. 3
Comparison of smears from Nutrison Energy multifibre tube feed (A and C) and pleural empyema from the right chest cavity (B and D) stained with hematoxylin‒eosin (upper row) and Congo red (lower row), scale bar 25 μm. Note that the Congo red-stained smears of both the control and pleural empyema samples contained similar rod-shaped Congo red-positive particles (inserts in C and D, scale bar 12,5 μm)
Chemical analysisChemicals and reagentsPapaverine at a concentration of 0.1 mg/mL was obtained from Cerilliant Corporation (Round Rock, Texas, USA) and was used as the internal standard. Normocaloric tube feeding solution was purchased from Nutricia (Erlangen, Germany). Analytical-grade methanol was obtained from Merck (Darmstadt, Germany).
Sample PreparationA 20 µL sample was introduced into a 2 mL reaction vial, spiked with 20 µL of papaverine and mixed with 960 µL of methanol. The mixture was vortexed for 30 s and centrifuged (5 min, 14000 rpm). Finally, 250 µL of the supernatant was transferred to a 1.5 mL glass vial for analysis.
Gas chromatography–mass spectrometryGas chromatography–mass spectrometry (GC/MS) analysis was performed via an Agilent 7890 gas chromatograph equipped with a 5975 C mass selective detector and an HP-5MS capillary column (30 m × 0.2 mm I.D., 0.25 μm film thickness) (Waldbronn, Germany). The injector was operated in splitless mode with an injection volume of 1 µL. The inlet temperature and helium flow rate were set to 280 °C and 1 mL/min, respectively. The oven temperature gradient program was as follows: hold an initial temperature of 160 °C for 1 min, ramp to 180 °C at 10 °C/min, then ramp to 220 °C at 5 °C/min, ramp to 270 °C at 15 °C/min, ramp to 300 °C at 10 °C/min, and finally hold for 5 min. The source and transfer line temperatures were 280 °C and 300 °C. The mass spectrometer was run in positive electron ionization mode at 70 eV. The acquisition range was set to 50–500 m/z in scan mode.
Analysis of the samplesAssuming that the pleural effusion from the present case was contaminated with the EN formula, a sample, the EN formula itself and one pleural effusion sample where EN could be excluded (negative sample) were analyzed. The resulting chromatograms were checked visually for characteristic differences. At 26 min, a signal appeared, which was exclusively found in the EN formula and in the case sample but not in the negative samples (Fig. 4).
Fig. 4
GC/MS chromatograms including a magnified view of the relevant retention time area: a) Nutrison energy multifibre tube feed; b) case sample; c) representative negative sample
Both peaks were identified as tricaprylin (1,2,3-propantriyl-trioctanoat) by using NIST 98 library [8], with quality scores of 91 and 87 (Fig. 5). The negative sample was analyzed for the presence of tricaprylin, and the results obtained indicated the absence of the analyte, thereby confirming that the circulating tricaprylin had not migrated from the blood into the thoracic effusion.
Fig. 5
Mass spectrum of tricaprylin
According to the manufacturer of the tube feed solution, the solution is composed of carbohydrates, fiber, protein, salt, various vitamins and lipids [9]. The latter also includes medium-chain triglycerides (MCTs) at a concentration of 9.2 mg/mL. One of these MCTs is tricaprylin, which is an organic chemical compound in which three hydroxyl groups of glycerol are esterified by octanoic acid. MCTs such as tricaprylin are fatty acids that can be obtained from coconut or palm kernel oil [10].
Comments (0)