A Structured Clinical Pathway Derived from Surgical Audit of VATS (Video Assisted Thoracoscopic Surgery) Lung Nodule Localization and Resections in Thoracic Oncology
Background
Lung nodules are commonly encountered in oncology practice, particularly in patients with solid organ tumors. Video-assisted thoracoscopic surgery (VATS) is frequently employed for their resection, but intraoperative localization remains a challenge, especially in resource-constrained settings. This study presents a novel algorithm for localizing and resecting lung nodules using VATS and evaluates its outcomes and validation.
Methods
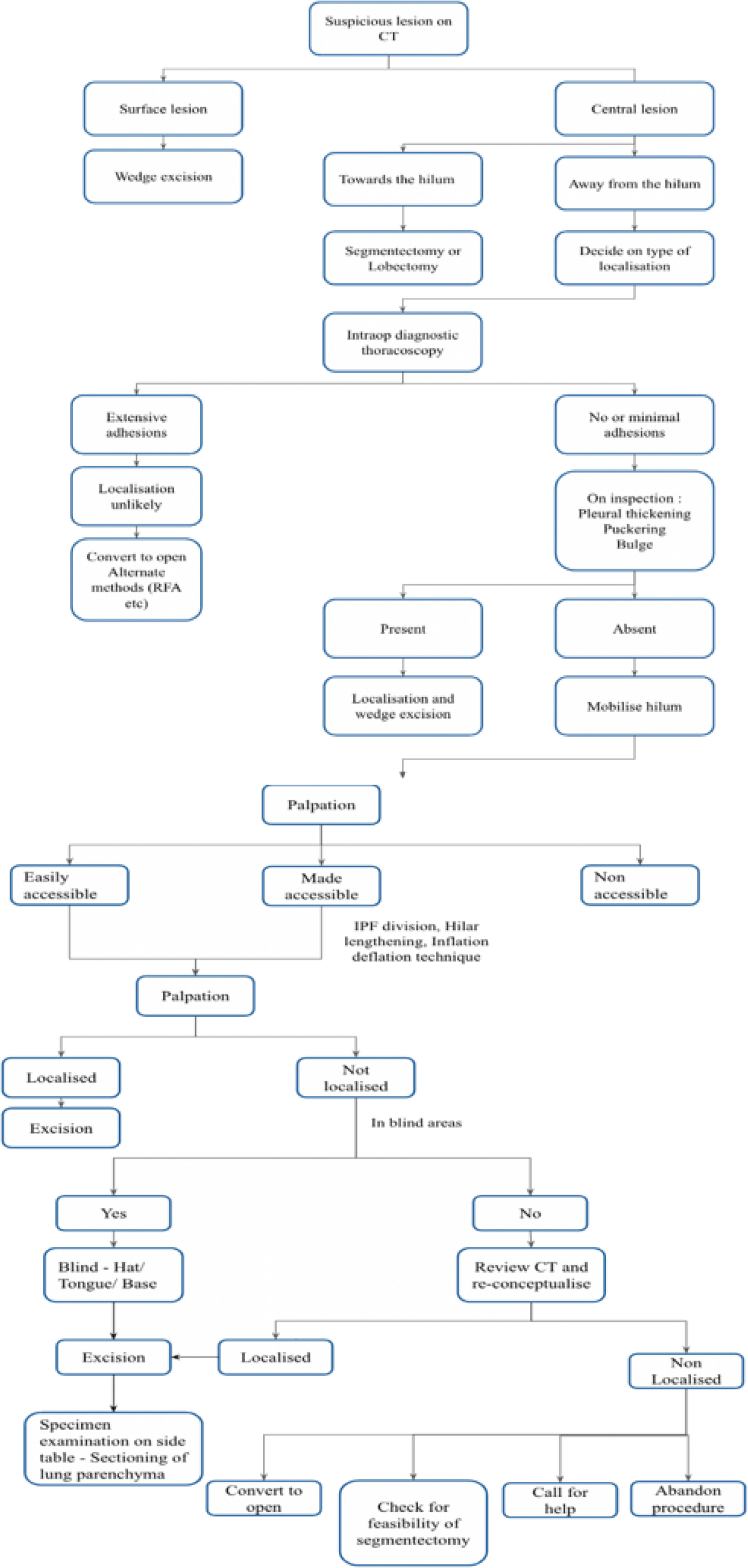
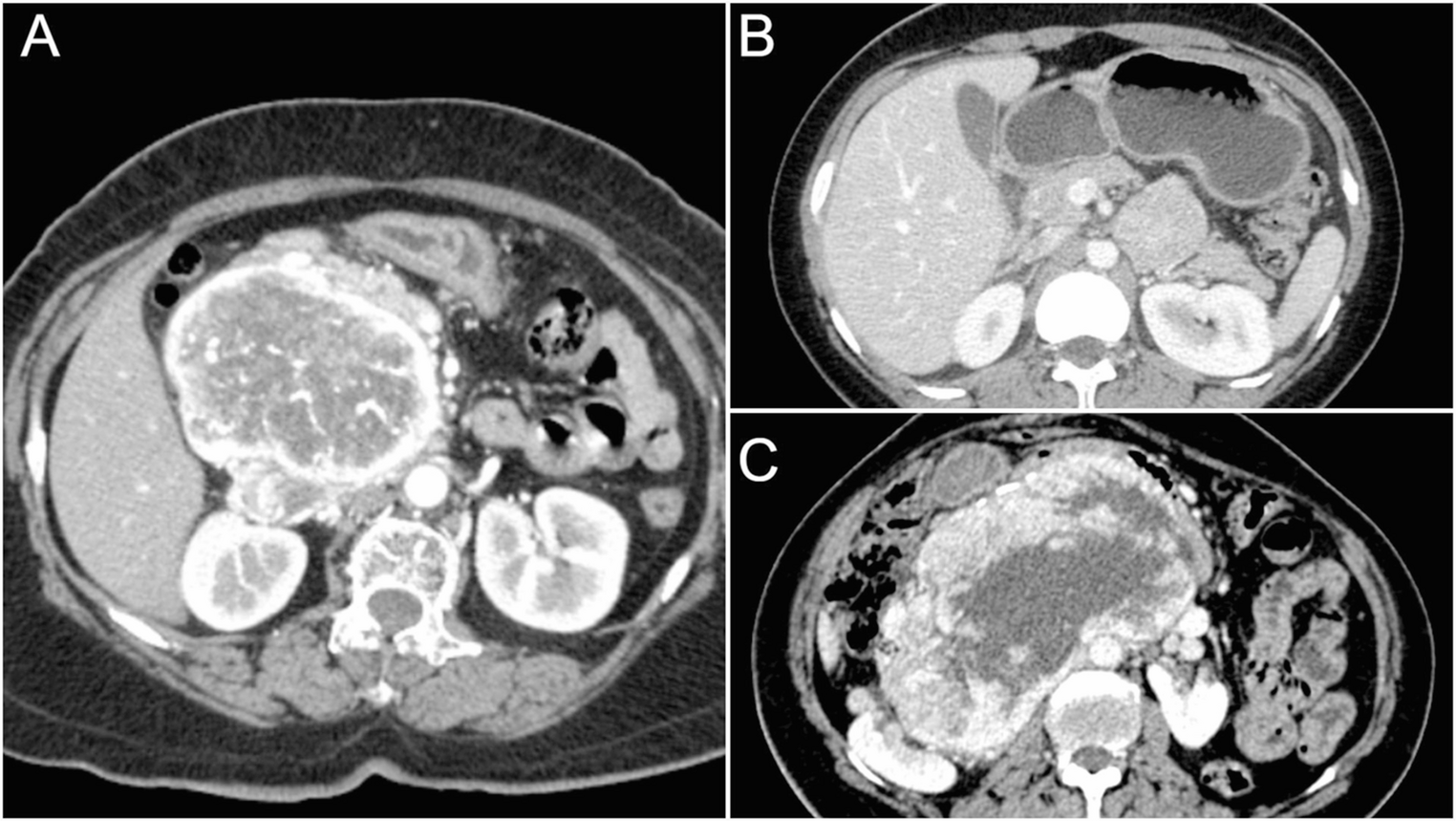
Patients who underwent VATS lung nodule resection by a single surgeon at oncology centers in South India between January 2019 and December 2024 were included. Nodules were classified as surface lesions, central lesions close to the hilum, or central lesions away from the hilum based on CT findings. The algorithm involved manual palpation, mobilization, and resection techniques tailored to nodule location. Outcomes, including sensitivity, accuracy, and resection margins, were analyzed.
Results
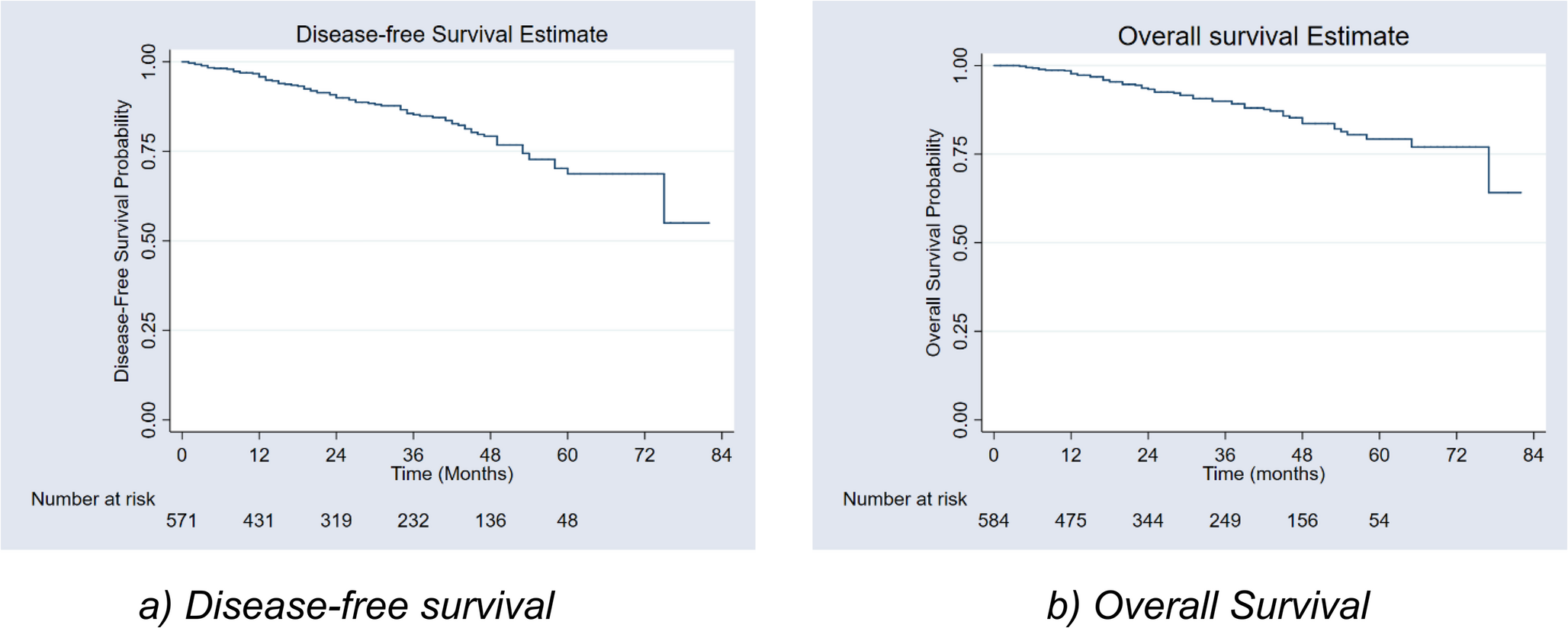
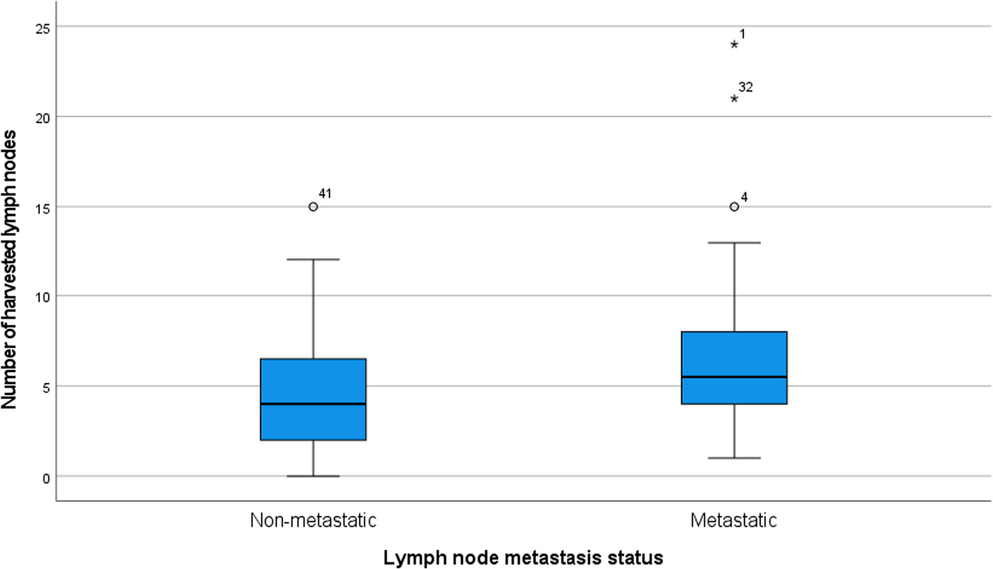
A total of 42 patients (25 females, 17 males) with a median age of 35 years underwent VATS resection. Nodules were predominantly located in the upper and lower lobes, with a median size of 2 cm. Histology included metastatic (32 cases) and non-metastatic (14 cases) nodules. The algorithm achieved a sensitivity and accuracy of 97.83% (45/46 nodules localized). All nodules were successfully resected with adequate margins, except one case requiring conversion to open surgery. Median procedure duration was 70 minutes, with a mean blood loss of 80 ml and a mean hospital stay of 4 days. Mild hemoptysis occurred in six patients, managed conservatively.
Conclusion
Our algorithm for VATS lung nodule localization and resection demonstrates high sensitivity and accuracy, making it a cost-effective and reliable method, particularly in resource- limited settings. It relies on manual palpation and radiological anatomy conceptualization, requiring an experienced surgeon. Further validation and integration with aided localization techniques are recommended to enhance its applicability.


Comments (0)