
Remember me
Sample size was calculated using the G*Power software (version 3.1.7; Heinrich-Heine-Universität, Düsseldorf, Germany). Based on the analysis, ten teeth per group was determined to achieve statistical significance, with an alpha level of 0.05, a beta power of 0.80, and an effect size of 1.39 [16].
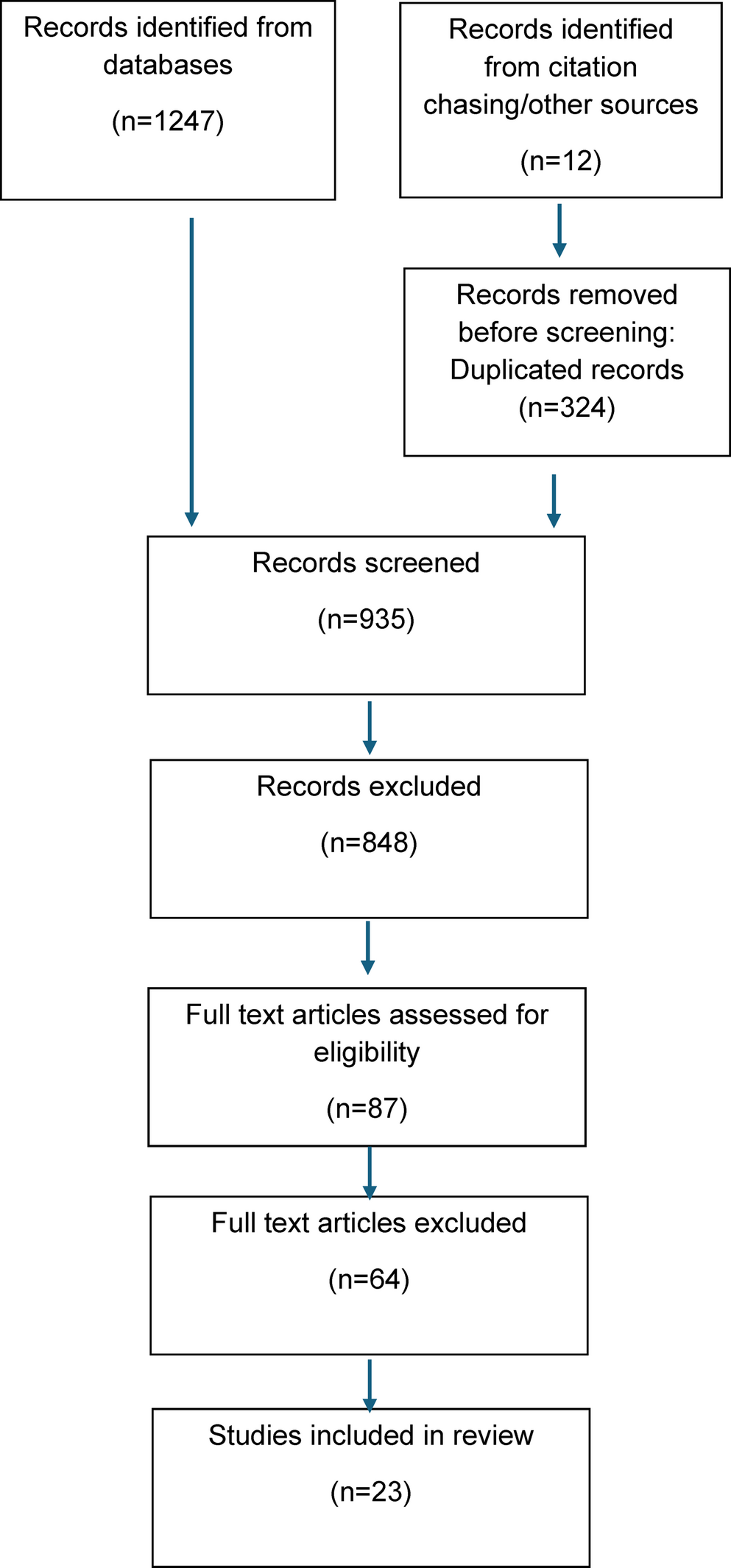
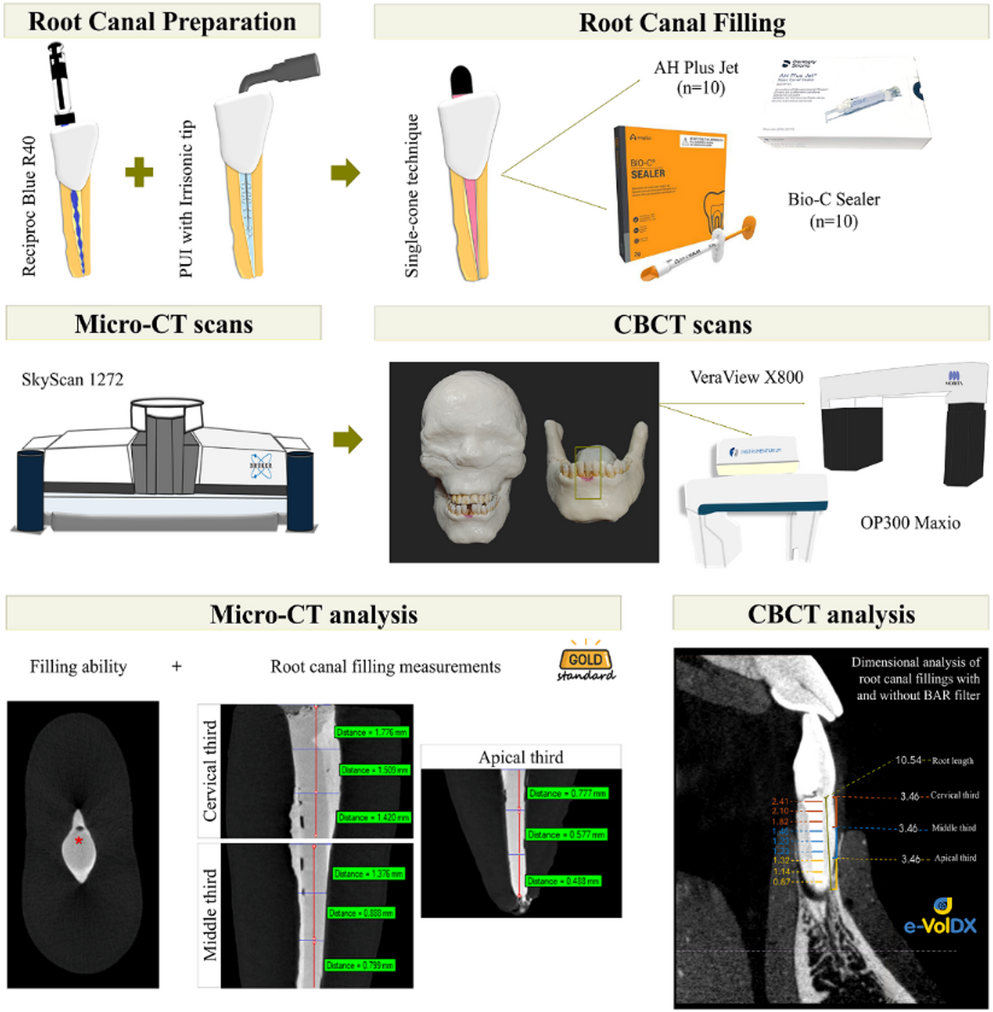
Selection of teethUnder the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, this study was approved by the institutional ethics committee (CAAE: 41916720.7.0000.5416 and 84582824.0.0000.5416). Twenty extracted human mandibular incisors with root canals classified as Vertucci’s type I [28] were selected. Inclusion criteria included complete apical formation, absence of root fractures, calcifications, previous endodontic treatment, or internal/external resorption. All root canals presented a long-oval cross-section, as determined by digital radiography (Kodak RVG 6100; Digital Radiography System, Marne-la-Vallée, France) and micro-CT scans (SkyScan 1272; Bruker MicroCT, Kontich, Belgium). The criteria for classifying the canals as long-oval were a buccolingual diameter 2 to 4 times larger than the mesiodistal diameter [29] at 9 mm from the root apex [5]. Measurements were performed using CTAn software (v. 1.15.4.0; Bruker MicroCT). A flowchart is presented in Fig. 1, outlining the sequential methodological steps followed in this investigation.
Fig. 1
Flowchart illustrating the methodological approach adopted in the study
Root Canal PreparationCoronal access was obtained using a #1012 diamond bur (Dentsply Sirona, Ballaigues, Switzerland). The root canals were explored with #10 C+ files (Dentsply Sirona), and the working length (WL) was determined by subtracting 1.0 mm from the point at which the file tip was visible in the apical foramen. Root canal preparation was performed with the Reciproc Blue R40 instrument (VDW GmbH, Munich, Germany) up to the WL, operated using the X-Smart Plus motor (Dentsply Sirona). Irrigation was performed with 6.0 mL of 2.5% sodium hypochlorite (NaOCl) (Ciclo Farma, Serrana, SP, Brazil) after each instrument, in 2 mL portions into the cervical, middle, and apical thirds of the root canal using a 30-G Navitip needle (Ultradent Products). The needle was positioned 2 mm short of the WL with back-and-forth movements under flow and aspiration. The final irrigation protocol consisted of 5 mL of 2.5% NaOCl, followed by 2 mL of 17% EDTA (Biodynamics, Ibiporã, PR, Brazil), and 5 mL of saline solution, all activated by passive ultrasonic irrigation (PUI) with an Irrisonic tip (Helse Ultrasonic, Santa Rosa de Viterbo, SP, Brazil). Finally, the canals were aspirated and dried with absorbent paper points (Dentsply Sirona).
Root Canal fillingAll root canals were filled using the single-cone technique with AH Plus Jet or Bio-C Sealer (n = 10 per group). R40 gutta-percha cones (VDW GmbH) were selected with a profilometer device (Profile Projector Nikon model 6 C-2; Nikon, Tokyo, Japan). Digital radiographs were taken to confirm the adaptation of the gutta-percha cones at the WL. For root canals filled with AH Plus Jet, 1 g of sealer was prepared by dispensing equal lengths of pastes A and B, then mixed for 30 s with a #24 metal spatula (Duflex, Juiz de Fora, MG, Brazil) on a glass slab (Golgran, São Caetano do Sul, Brazil) until a homogeneous consistency was achieved [30]. The sealer was applied using a #40 Lentulo spiral (Dentsply Sirona) connected to a low-speed motor (Micromotor N270 with contra-angle, Dabi-Atlante, Ribeirão Preto, SP, Brazil), positioned 2 mm short of the WL [7]. Bio-C Sealer was injected into the root canals using syringes and plastic needles positioned 4 mm short of the WL according to the manufacturer’s instructions. The syringe plunger was pressed lightly until the sealer flowed back into the cervical third, indicating complete filling of the root canals [7]. The R40 gutta-percha cones were coated with the respective sealers and inserted to the WL. Excess gutta-percha was removed from the cervical third and compacted vertically with a Paiva #2 plugger (Golgran). Final digital radiographs were obtained in both mesiodistal and buccolingual directions to confirm the absence of voids and the uniformity of fillings. The root canals were restored with Coltosol (Vigodent, Rio de Janeiro, RJ, Brazil), and the specimens were stored at 37 °C and 95% relative humidity for one week to allow complete sealer setting [31].
Micro-CT acquisitionTo obtain the gold-standard reference for comparisons with CBCT scans, the teeth were individually scanned using a high-resolution micro-CT device (SkyScan 1272; Bruker MicroCT). The scanning parameters were: voxel size of 9 μm, 1-mm aluminum filter, exposure time of 87 ms, 180° rotation, rotation step of 0.5°, 80 kV and 300 µA.
CBCT acquisitionFor CBCT imaging, an anthropomorphic model consisting of a skull and a fully dentate mandible was used. The phantom was coated with Mix-D, a material designed to simulate X-ray attenuation similar to human soft tissues, and also served to create a tongue model [31]. The left mandibular central incisor of the dry mandible was carefully removed, and the prepared teeth were individually positioned in the empty sockets. Two CBCT devices were used: VeraView X800 (J Morita, Tokyo, Japan) and OP300 Maxio (Instrumentarium Dental, Tuusula, Finland). For the VeraView X800, images were acquired with a voxel size of 0.08 mm, exposure settings of 70 kV and 5 mA, and a field of view (FOV) of 40 × 40 mm. For the OP300 Maxio, acquisition was performed with a voxel size of 0.08 mm, 90 kV, 8 mA, and an FOV of 50 × 50 mm.
Micro-CT image analysisThe micro-CT images were reconstructed using NRecon software (v1.6.3, Bruker MicroCT) with specific artifact correction adjustments, including beam hardening, ring and smoothing corrections, according to the sealer used (AH Plus Jet or Bio-C Sealer). For quantitative analysis, a region of interest (ROI) corresponding to the root canal space was defined. From this region, the total volume (mm³) of the filling material, as well as the percentage of filled areas (%) and voids (%), were calculated. Global image segmentation was performed using the automatic thresholding plug-in of CTAn software, with manual adjustments when necessary.
The micro-CT images were also used to establish the diameter of the root canal filling material and to detect possible measurement distortions for canals filled with either AH Plus Jet or Bio-C Sealer. The analysis was performed in the sagittal plane using CTAn software to assess the buccolingual dimensions of the filling material at the cervical, middle, and apical thirds of the root canal. For each specimen, the sagittal reconstruction plane was carefully adjusted to pass through the center of the root canal filling and aligned with the long axis of the root. The same anatomical references and plane orientation were used for all specimens and imaging modalities. These data served as the gold standard for comparisons with CBCT-derived measurements, obtained with and without the BAR filter. The examiner responsible for the micro-CT measurements was not involved in evaluations of the CBCT images.
CBCT image analysisCBCT images were analyzed using e-Vol DX (CDT Software, Bauru, SP, Brazil) by three examiners, who were instructed to perform detailed measurements across the cervical, middle, and apical thirds of root canals filled with AH Plus Jet or Bio-C Sealer. A calibration process was performed using random images, in which the examiners were shown how to analyze the images under the same conditions. Subsequently, each examiner individually analyzed four random images, including variations of CBCT devices, root canal sealers and application or absence of the BAR filter. The images used in the calibration process were not included in the final evaluation. The intraclass correlation coefficient (ICC) indicated good agreement between the examiners.
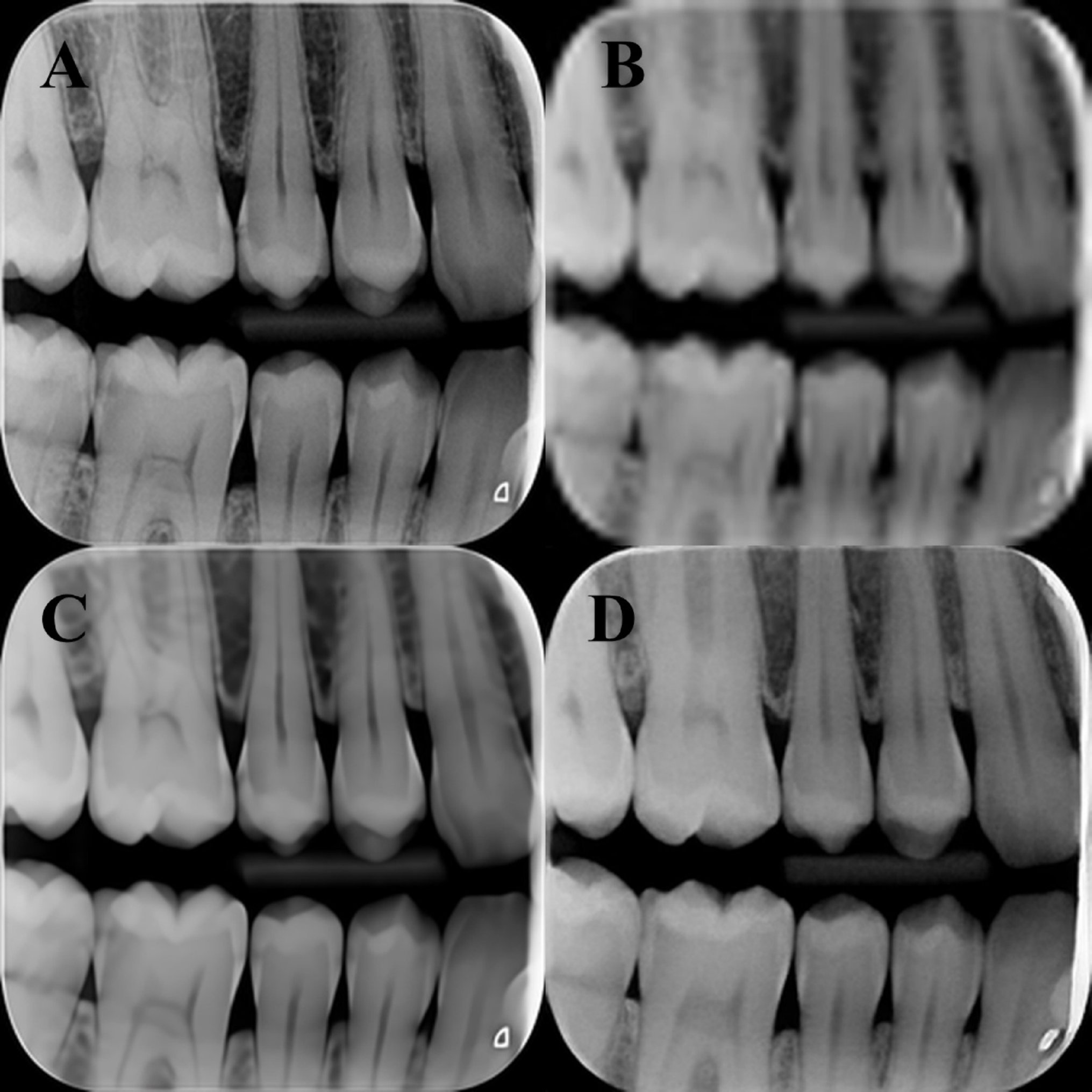
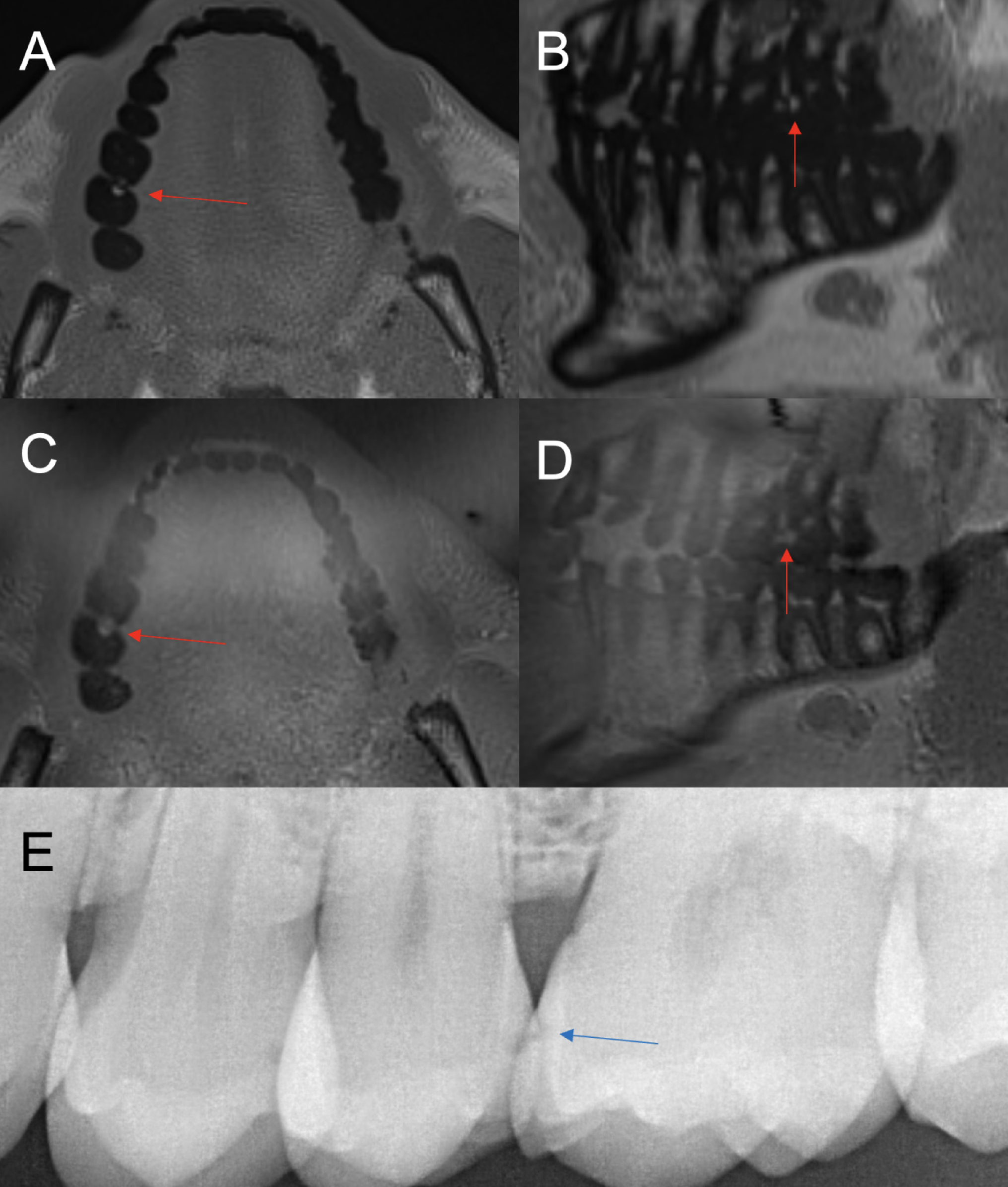
Once the examiners were familiarized with the measurement parameters and calibrated, the CBCT images were analyzed. The diameter of the root canal fillings was measured on sagittal reconstructions obtained from both CBCT devices, under two conditions: with and without the BAR filter. Sagittal reconstruction planes were defined using the same criteria adopted for the micro-CT analysis, being aligned with the long axis of the root canal and positioned to pass through the center of the filling material, thus ensuring that measurements were obtained from corresponding anatomical locations across CBCT and micro-CT images. To standardize the evaluation, each root was divided into three segments (cervical, middle, and apical) based on the location of the filling material. The measurements across the three segments were performed in triplicate. This approach ensured that all examiners assessed the root canals in a standardized manner [32]. All images were analyzed on a 25-inch color LED monitor with a resolution of 2560 × 1080 pixels, in a low-light and quiet room. To minimize visual fatigue, a maximum of five CBCT volumes were evaluated per day, with at least 24 h between evaluation sessions. To assess intra-examiner reproducibility, 30% of the sample was randomly selected and reanalyzed after a 30-day interval following the initial evaluation. Dimensional measurements on CBCT and micro-CT images were performed as illustrated in Fig. 2.
Fig. 2
Sagittal reconstructions of a mandibular central incisor from the sample, illustrating buccolingual dimensional measurements of the filling material. Micro-CT images (left) served as the reference standard, while CBCT images (right) were analyzed to detect dimensional distortions in the cervical, middle, and apical thirds of the root canal, with and without application of the BAR filter
Statistical analysisStatistical analyses were performed using GraphPad Prism 9 (GraphPad Software. San Diego, CA, USA) and SPSS software (v24.0, IBM Corp., Armonk, NY, USA). The intraclass correlation coefficient (ICC) was calculated to assess intra-examiner reproducibility and inter-examiner reliability for CBCT analysis. Data normality was verified using the Shapiro–Wilk test. An unpaired t-test was used to compare the filling ability of the sealers based on micro-CT measurements. Repeated measures ANOVA followed by Tukey’s post hoc test was applied for multiple comparisons between the reference measurements (micro-CT) and those obtained from CBCT images with and without the BAR filter. A significance level of 5% was adopted for all analyses.
Comments (0)