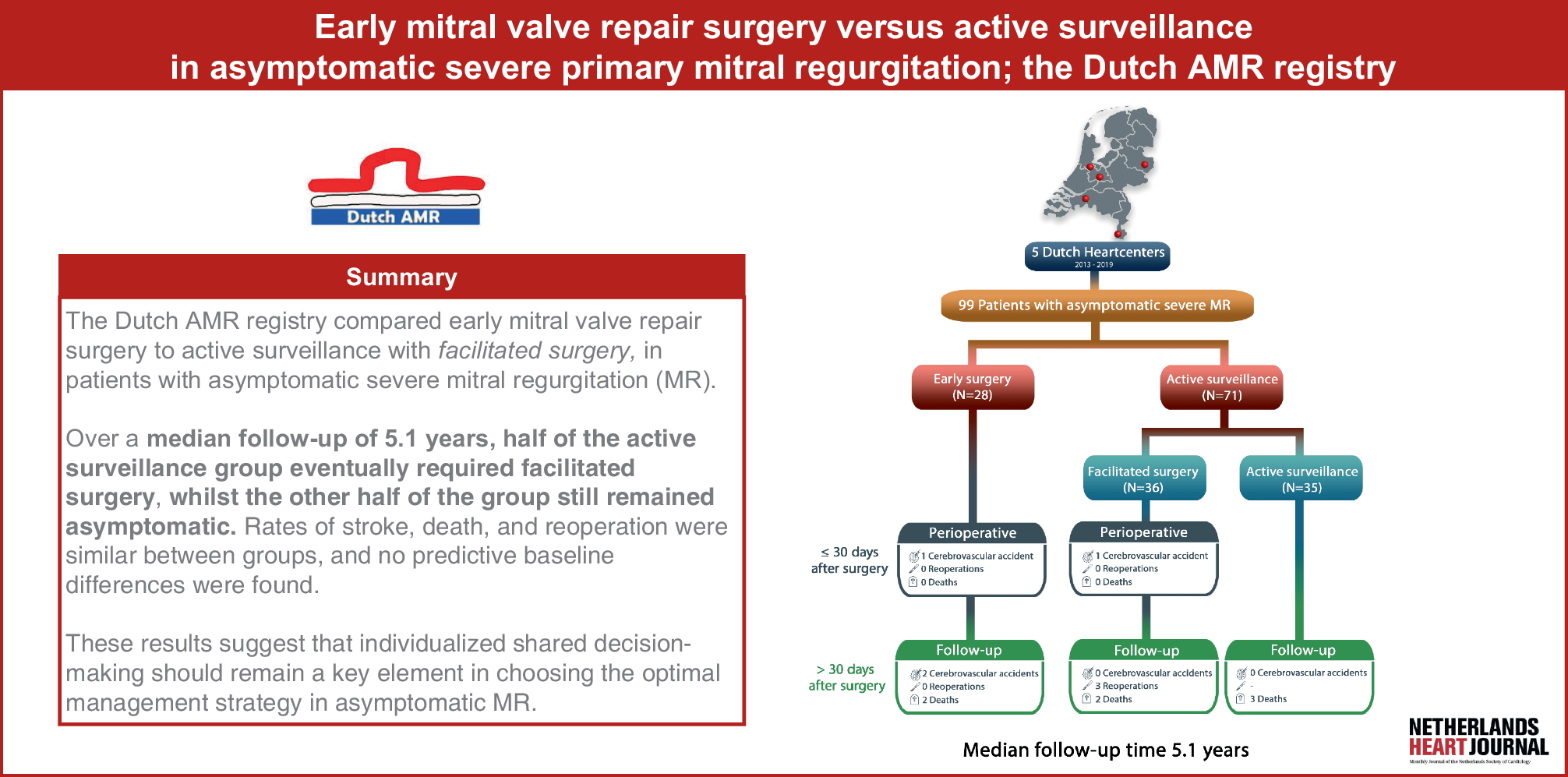
The findings of the multicenter Dutch AMR registry can be summarized as: (I) After a median follow-up time of 5.1 years, 51% of patients with asymptomatic severe MR developed a surgical indication and underwent facilitated surgery, (II) overall incidence of primary endpoints were 3 CVAs and 2 deaths in the early surgery group (n = 28) versus 1 CVA, 5 deaths and 3 reoperations in the active surveillance population (n = 71), (III) clinical endpoints were comparable between the early and facilitated surgery strategy, except for the incidence of CVAs during follow-up (only in the early surgery group; n = 2) and reoperations during follow-up (only in the facilitated surgery group; n = 3) and (IV) there were no differences in baseline additional testing parameters, suggesting no clear targets for upfront stratification.
These results corroborate the findings of Rosenhek et al. [6, 11], demonstrating that active surveillance can be safely accomplished in asymptomatic MR patients (n = 132) since half of the patients remained asymptomatic throughout the follow-up period, without meeting guideline indications for surgery. Additionally, the reoperation rate within the facilitated surgery group (5.3%) in this study was comparable to ours (8.3%). Our results, however, differ from a Belgian cohort (n = 192) where 90% of patients necessitated surgery within a median follow-up time of 8.5 years [12]. Additionally, the mortality rates in their active surveillance group (46.2%) and early surgery group (11.2%) were significantly higher than those observed in our cohort. These differences may be explained by the longer follow-up and the inclusion of patients with AF [16]; which was an exclusion criterion in our study. The largest cohort on this topic, comprising 2,097 patients [9], revealed improved survival rates for the early surgery group (86%) compared to active surveillance (69%), underscoring higher mortality rates compared to our study.
Active surveillance patients who required facilitated surgery during follow-up
After half of the active surveillance group underwent facilitated surgery, all reoperations in our study were in this group, raising questions about whether delaying surgery affects MVR success (100% success in early surgery vs. 92% in facilitated surgery). The reoperations involved patients with Barlow’s disease (n = 1), anterior leaflet prolapse (n = 1), and posterior leaflet prolapse (n = 1). A possible explanation for the exclusive incidence of reoperations in the facilitated surgery group is that delaying surgery may allow for further progression of MV degeneration and LV remodeling. As severe MR persists over time, structural changes in the mitral apparatus and LV can occur, potentially making repair technically more challenging and increasing the likelihood of recurrent MR or repair failure. On the other hand, in clinical practice, early surgical intervention is often performed in patients with less advanced diseases and may therefore be associated with more durable repairs and a lower risk of reoperation. However, given the small number of reoperations in our study, the findings should be interpreted with caution and considered hypothesis-generating rather than definitive.
Furthermore, half of the active surveillance patients developing a surgical indication remained asymptomatic, and all patients developing AF reported no symptoms. This highlights the importance of vigilant monitoring [17].
Perioperative and long-term outcome after early and facilitated surgery
In the perioperative period, one patient in each group experienced a CVA, with no POAF. Interestingly, both CVAs during follow-up (> 30 days post-surgery) occurred in the early surgery group, though no patients had residual symptoms or documented AF, raising questions about the cause of these events. Given the small sample size of this study, it is not possible to answer these questions, as these occurrences could also be attributed to chance. No perioperative deaths occurred, though two deaths in each group were recorded during follow-up.
Baseline tests (CPET ± VO2 max, Holter monitoring, CMR) showed no differences between groups, indicating similar preoperative status and limiting predictive stratification. Most patients in both groups reported good quality of life; however, a few (early surgery: 3; facilitated: 1) reported feeling worse postoperatively. All patients under continued active surveillance reported well-being without complaints, raising questions about the necessity of early surgery, as they may have remained asymptomatic without intervention. This suggests that subjective well-being, alongside further diagnostics, should play a role in shared decision-making on treatment strategies [18].
Limitations
Our study has limitations due to its small sample size, which hinders robust statistical analysis and requires cautious interpretation of results; therefore, the reported outcomes remain exploratory. Initially aiming for 250 participants, we faced difficulties in randomizing asymptomatic patients, leading to a low enrollment rate and making future RCTs unlikely. We may explore emulation target trial settings for better insights. Given the long timeline since the Dutch AMR study began, we opted to close the study and report outcomes based on the available sample [13]. Additionally, the lack of randomization may have introduced selection bias, as treatment strategies were chosen based on patient and cardiologist preferences. A further challenge is accurately determining the onset of severe MR, especially in asymptomatic patients who may be diagnosed incidentally. This could lead to an underestimation of the asymptomatic period before surgery. Another limitation is the incomplete collection of baselines NT-proBNP levels, which were missing for approximately 75% of study participants. As a result, we were unable to assess whether baseline NT-proBNP levels were associated with the likelihood of becoming symptomatic or the need for facilitated surgery during follow-up. Nor were we able to define the value of consecutive NT-proBNP measurements in this population.
This limitation stems from the pragmatic approach of our study, which followed routine clinical practice rather than a formal, protocol-driven research framework. While this approach increases the real-world relevance of our findings, it also led to incomplete data capture for certain variables, including biomarkers like NT-proBNP. In the absence of dedicated research funding or infrastructure, systematic testing and standardized follow-up were not consistently feasible. Consequently, our ability to perform detailed subgroup analyses or assess the value of additional prognostic indicators was limited. We acknowledge this as an inherent trade-off in pragmatic research, and it should be considered when interpreting our results.
Another important remark is that defining truly asymptomatic patients with severe MR is challenging, as clinical symptoms and AF are not always systematically assessed. Many previous studies have relied on observational data from registries or nonrandomized trials conducted in expert centers, where diagnostic protocols, such as Holter monitoring or exercise testing, were not consistently applied [19]. This lack of uniformity raises concerns about patient classification and may have influenced study outcomes, limiting the generalizability of results. Given the increasing prevalence of MR due to an aging population, it is crucial to adopt strict, standardized diagnostic criteria and refer all patients with severe MR to specialized heart teams for individualized evaluation. By adhering to guidelines and ensuring systematic assessments, we can improve both patient care and the quality of future research. As such, comparisons with prior studies should be made with caution.

Comments (0)