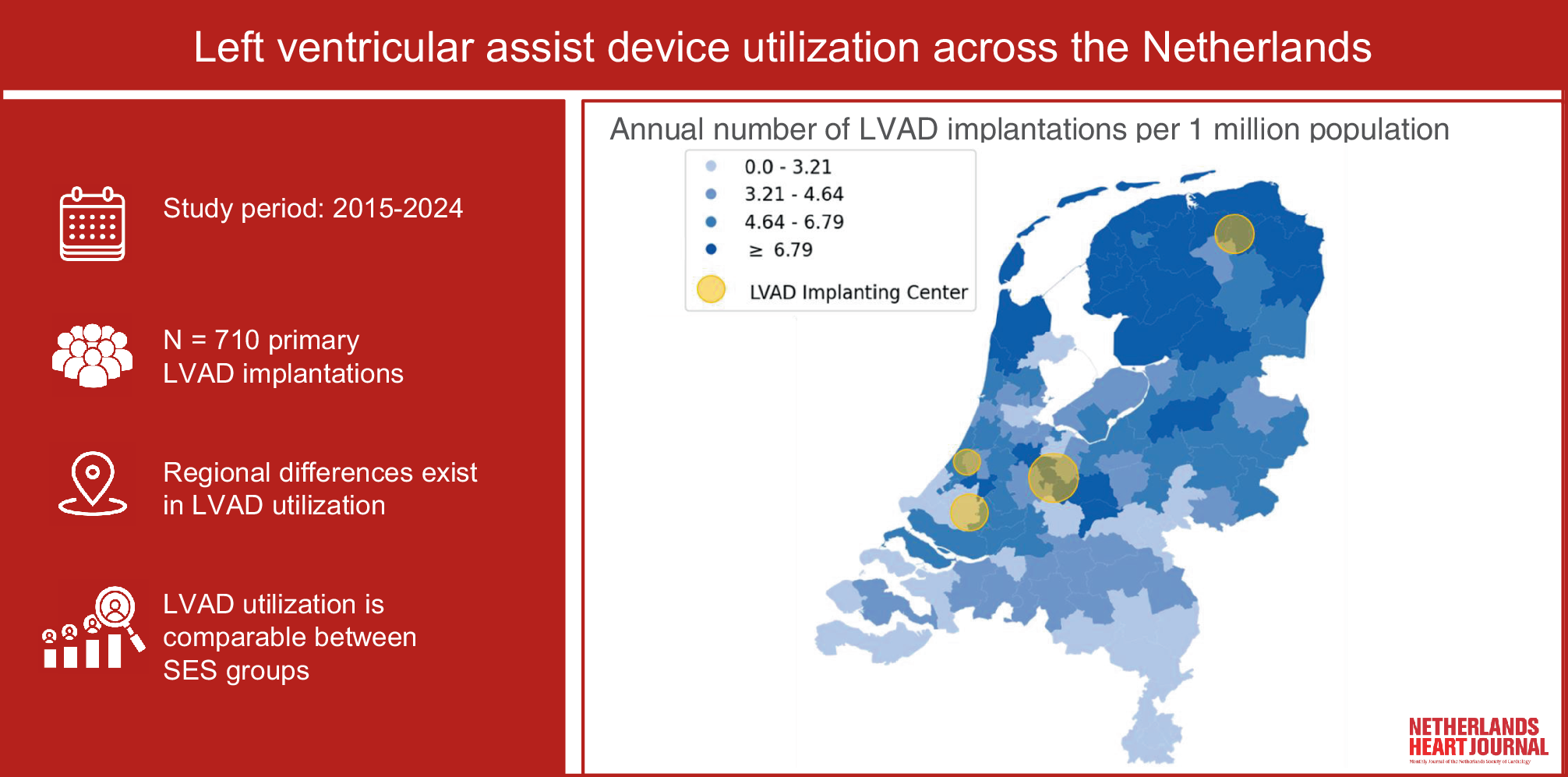
In this descriptive study, we visualized the regional distribution of LVAD implantations in the Netherlands from 2015 to 2024. Also, we compared implantation rates between different levels of SES. We noted differences in LVAD utilization between postal code areas, with a higher frequency of LVAD implantation per 1 mio. population in northern and central regions. Additionally, this study demonstrates that there is no significant relation between distance to the implantation center and implantation frequency. Similar to the higher implantation rate, the cardiovascular mortality was also high in the northern regions. In contrast, areas in the southern parts of the country show substantially lower rates of LVAD implantation, while cardiovascular mortality was also high in southern provinces. Here, it should be mentioned that although related and therefore showing the distribution of cardiovascular diseases in the Netherlands, heart failure is only one of the cardiovascular diseases that can cause a high cardiovascular mortality.
The average annual rate of LVAD implantation in the Netherlands corresponds to 4.6 per 1 mio. population. As compared with a survey by the European Society of Cardiology, the Netherlands ranks among the countries in Europe with the highest implantation rates per 1 mio. population. Compared to its neighboring countries, the Netherlands ranks lower than Germany (13.9), but still higher than Belgium (4.1), Denmark (3.2), and the United Kingdom (0.6) [17]. This may be partly explained by the lack of reimbursement for destination therapy for LVADs in some of these countries and long waiting times for heart transplantation in the Netherlands, necessitating long-term LVAD therapy. Although the implantation rate in the Netherlands is high by European standards, there is room for improvement in the utilization of LVAD therapy, as it is expected that a proportion of patients with advanced heart failure, the fifth leading cause of death in the Netherlands for years, will be overlooked. The underutilization of LVAD therapy, a potentially life-saving therapy in these patients, has been previously described [18]. Strikingly, research using market data across European countries showed that the utilization of LVAD devices does not mirror the increase in heart failure mortality [19]. Therefore, raising awareness for recognition of advanced heart failure and timely referrals remains critical.
Low SES is associated with an increased incidence of heart failure, related adverse events, and mortality [20]. Moreover, research shows that lower SES is also associated with lower utilization of potentially life-saving device therapy, including CRT and ICD [12]. However, studies have not yet assessed the influence of SES on LVAD utilization. In our study, no significant differences were observed in LVAD utilization between areas in different SES categories. These results suggest that the use of LVAD therapy in the Netherlands was not influenced by SES. Nevertheless, it is unknown what the need for LVAD therapy is for different SES scores. This need could be different over the different SES groups, for example, due to the association of low SES with increased incidence of heart failure and differences in therapy, possibly causing an underestimation of the effect of SES on implantation frequency [12, 20].
The observed geographic differences in LVAD utilization may be explained by several other factors, such as the level of awareness of referral criteria among physicians and ability to identify optimal timing of referral to advanced heart failure centers. Physicians have been found to overlook potential LVAD candidates due to older age or comorbidities and are still adhering to previously strict criteria for heart transplantation [21]. Timely referral is a critical factor in improving outcomes for advanced heart failure patients who may benefit from LVAD therapy. Particularly for relatively younger heart failure patients aged < 70 years, who were initially eligible candidates, the disease progression and comorbidities can make a patient ineligible for both transplantation and LVAD therapy [9, 22]. LVAD utilization could also depend on the patient’s awareness of available advanced HF treatment options. Patients generally rely on their treating physician for this information [23]. Furthermore, physicians should have sufficient clinical confidence in LVAD therapy in eligible patients [10]. Therefore, understanding the awareness of referral criteria among health care providers and patients, along with reasons behind both referral and non-referral, could offer valuable context for regional utilization of LVAD therapy. In future research, temporal analysis of the annual implantation rate at the regional level can show changes over time. Such year-by-year information may provide actionable insights for improving access to LVAD therapy.
Limitations
For interpretation of the results, it should be noted that in this study, the most recent available residential data was used to determine LVAD implantation frequency. Additionally, referrals to implanting centers outside the Netherlands were not taken into account, which could potentially lead to underestimation of the number of implantations. However, considering the healthcare reimbursement system in the Netherlands, this number is expected to be negligible.
Also, in this study, we used the median SES-WOA score per 2‑digit postal code area. Within these areas, differences in SES-WOA scores may exist at the individual level. For a more detailed analysis of the relation between individual LVAD implantation and SES-WOA score, household SES-WOA scores could be reviewed.
Furthermore, the observed regional utilization of LVAD therapy may also be impacted by several other related factors. These could be patient-related factors, such as heart failure incidence, corresponding age, comorbidities, and logistical factors such as mobility. Although detailed information about these topics was not available for analyses in this study, these factors are not likely to be reversely correlated to cardiovascular mortality and would therefore not explain the geographical inequity observed in our study. A general impression of baseline characteristics of patients implanted with an LVAD between 2016 and 2020 in the Netherlands is provided by Damman et al. [7]. Other factors that could have impacted LVAD utilization may be linked to physician awareness, referral patterns, and inter-hospital agreements and collaborations. An example of the latter can be the use of a shared care model as described by Drost et al. [24].
Overall, utilization of LVAD therapy may depend on many factors and results from a comprehensive interaction between the referring center, implanting center, and the patients’ needs and preferences, which are not all covered in the data presented in this study. Therefore, conclusions on causal relationships could not be drawn. The use of advanced heart failure data at the regional level would have enabled us to study the relation between advanced heart failure incidence and LVAD utilization. Unfortunately, this data was not available. To allow for such analyses, we recommend further improving the availability and completeness of detailed heart failure databases at the national level, such as the Netherlands Heart Registration and Heart4Data [25, 26].

Comments (0)