
Remember me

The impact of chemotherapy agents on human ovary occurs via several different mechanisms First, they induce apoptotic death of oocyte and granulosa cells of primordials and growing follicles by exerting direct cytotoxic effects and/or causing additional harmful effects on ovarian stroma and vascular structures (Figs. 1 and 2) [5]. Among chemotherapy drugs, alkylating agents cause the most extensive ovarian damage and follicle destruction. Moreover, these agents induce genomic damage in somatic cells of dormant primordial and growing (secondary) follicles and cause massive follicle loss [5,6,7,8]. Second mechanism is the vascular and stromal damage related to chemotherapy-induced cytotoxicity. Certain chemotherapy drugs such as platinium group preferentially target vascular structures in the cortical and medullary portions of the human ovary, resulting in obliteration, fibrosis, and decreases in vascular endothelial growth factor (VEGF) and microvascular intensity [8,9,10,11]. The resultant decrease in ovarian vascularization may impair blood supply, aggravating follicle loss further and accelerating ovary aging. Disruption in ovarian vascular supply sometimes can be so severe that it can even be detected on doppler examination of ovarian vascularity as shown by a study in which young breast cancer patients treated with anthracyclines and taxanes. Ovarian blood flow was significantly reduced shortly following chemotherapy: Resistive index (RI) decreased by 52.5% and pulsatility index (PI) decreased by 24.2%. The mean ovarian size declined by 19.08% along with reduction in serum anti-Müllerian hormone levels [12].
Fig. 1
Conventional chemotherapy drugs used in the treatment of breast cancer and their mechanisms of action according to the cell cycle stage. Drugs that exert their anti-proliferative effects at a specific cell cycle stage, such as mitosis-specific taxanes and S-phase-specific antimetabolites, are less detrimental to the ovary than cell cycle–nonspecific alkylating agents, which cause more widespread ovarian destruction. ROS, reactive oxygen species; 5-FU, 5-fluorouracil; MTX, methotrexate
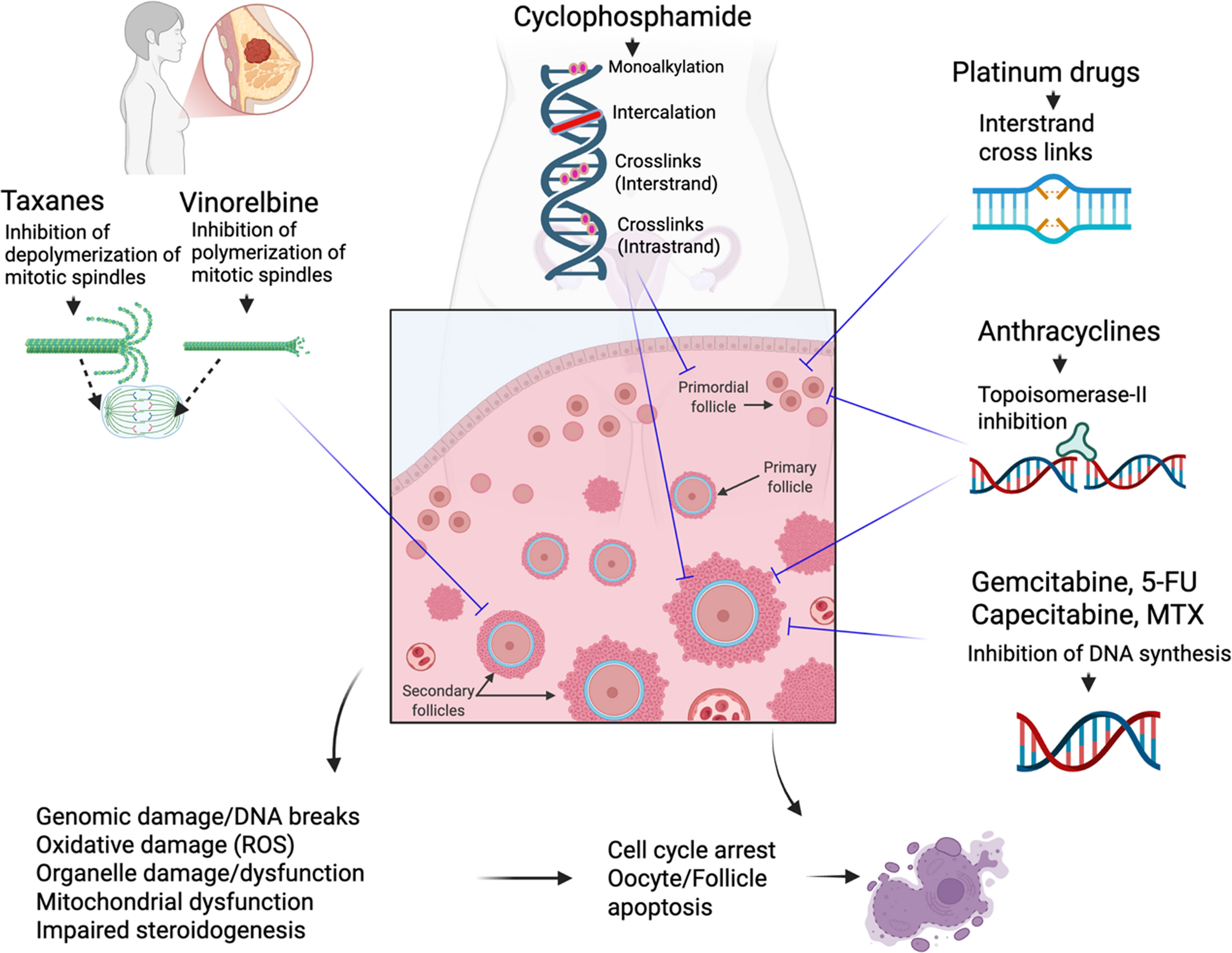
Fig. 2
Overview of the proposed mechanisms by which conventional chemotherapy and targeted anticancer agents compromise ovarian function. The central illustration depicts a cross-section of a human ovary, demonstrating follicles at different stages. Black dashed arrows trace pathways known to be affected by conventional cytotoxic drugs, whereas red dashed arrows denote effects reported for targeted agents. Symbols depicting a rat indicate findings derived predominantly from animal models, while the human figure denotes mechanisms supported by human clinical, histological or translational data
The third mechanism of follicle loss is the “burn-out” phenomenon, characterized by the massive premature activation of dormant primordial follicles. Normally, the PI3K/Akt/mTOR signaling pathway, which drives follicle activation, is held in check by local inhibitory factors, including anti-Müllerian hormone (AMH) secreted by the growing follicle pool [13]. Chemotherapy-induced destruction of these anti-Müllerian hormone-producing growing follicles leads to a precipitous drop in local anti-Müllerian hormone levels. This reduction disinhibits the PI3K pathway, resulting in the downstream phosphorylation and nuclear export of the transcription factor FOXO3a. Consequently, the inhibitory clamp on the primordial follicles is released, triggering their massive entry into the growing pool and subsequent atresia due to the toxic environment [14]. Systemic administration of anti-Müllerian hormone attenuated cyclophosphamide-induced follicle loss by decreasing phosphorylation FOXO3A and possibly inhibiting PI3K pathway in mouse ovary [15]. It is important to note that this mechanism has been primarily established in rodent models, particularly with cyclophosphamide. Evidence in humans remains limited and controversial. While some in vitro human ovarian cortical studies support PI3K pathway upregulation following chemotherapy exposure, in vivo human ovarian xenograft studies suggest that direct DNA damage (apoptosis) rather than “burn-out” is the dominant mechanism of primordial follicle loss in humans [5, 16].
The forth proposed mechanism, at least conducted with mice ovaries, explains the different mechanisms of follicle loss. For example, while cisplatin exposure causes oocyte-specific damage, doxorubicin induces more selective damage to the mitotic granulosa cells of secondary follicles [14].
As an index drug of alkylating category cyclophosphamide is included in several combined regimens (CEF, CMF, AC, AC-T) in the treatment of breast cancer. Cyclophosphamide itself is a pro-drug which undergoes a a 4-hydroxylation step in the liver and then spontaneous ring opening to form phosphoramide mustard and acrolein. While the former is primarily responsible for gonadotoxic effects, the latter causes urinary toxicity. The formation of guanosine adducts that prevent DNA replication and damage to mitochondria and other organelles within cells are the primary mechanisms of the cyclophosphamide-induced cellular cytotoxicity [7, 16]. Cyclophosphamide is metabolically activated by CYP2B6 enzyme and induces cellular death by forming DNA adducts, in particular, the interstrand DNA crosslink, through formation of the active metabolite, phosphoramide mustard. The drug primarily alkylates the N-7 position of guanine and forms 67% phosphotriester monoadducts, 26% N-7-guanine monoadducts, and 6.7% N-7-guanine-N-7 guanine interstrand crosslinks. Even though interstrand crosslinks comprise only 5–10% of all adducts formed by alkylating agents, these adducts are the most physiologically relevant because of their ability to block DNA replication and their association with cytotoxicity [17, 18]. In human fetal ovaries xenografted to immune deficient mice cyclophosphamide caused massive apoptosis of oocytes and granulosa cells of primordial follicles starting as early as 24 h after administration of the drug as an in-vivo real time histomorphometric evidence of the gonadotoxicity of the drug [5].
Chemotherapy drugs used in treatment of breast cancer have ovarian toxicity profiles that vary according to their cell cycle-specificity toxicity (Figs. 1 and 2). For instance, the alkylating agents and anthracyclines (non-specific cell-cycle agents) are capable of impacting cell at every stages of cell cycle. Therefore these drugs induce more widespread damage to the ovary. By contrast, cell-cycle-specific agents (e.g., 5-fluorouracil and methotrexate) could be more likely to cause damage to the preantral and antral follicles than primordial follicles due to their higher mitotic rate and metabolic demand. Although there is still no direct in-vivo histomorphometric evidence in human ovary, the evidence supporting this notion came from a mouse study, which demonstrated that multidose 5-FU treatment resulted in dramatic and progressive atresia of growing follicles and a profound decrease in ovarian volume due to reduced corpus luteum counts. Primordial follicle numbers were not affected and therefore, 5-FU is unlikely to cause permanent infertility when administered to women of pre or reproductive age. Furthermore, this study suggests that depletion of the growing follicle population is insufficient to stimulate follicle activation and primordial follicle depletion [19].
The Risk of Ovarian Failure and Amenorrhea after Receiving Conventional Chemotherapy Drugs for Breast CancerAlkylating RegimensCMF (cyclophosphamide, methotrexate, and 5-fluorouracil) is one of the most commonly employed chemotherapy regimen of alkylating category. The incidence of amenorrhea following receiving CMF regime widely changes from 0% to 97% in premenopusal women [20, 21] due to heterogeneity in patients’ age, duration of treatment and follow-up [4]. Younger patients are more likely to have higher ovarian reserve and retain more residual ovarian function after completion of chemotherapy. As an example, Bines et al. reported that ovarian failure incidence after the CMF regime is lower in patients younger than 40 (respectively, 40% vs. 76%) [22]. The amenorrhea risk is higher in older patients because of age-related decline in their ovarian reserve. In another series, none of the 25 patients younger than age 35 developed amenorrhea after six courses of CMF, whereas 33.3% and 80% of the patients at ages between 36 and 40 and 41–45, respectively, developed amenorrhea after receiving the same regimen [20]. Moreover, temporary amenorrhea (hazard ratio = 1,96) and CMF X 6–7 (hazard ratio = 2.03) are related to premature menopause [23].
CEF or FEC (Cyclophosphamide, Epirubicin, and 5-Fluorouracil) is another alkylating regimen used for breast cancer treatment. One study showed that the risk of amenorrhea after CEF appears to be significantly higher compared to CMF (76% vs. 64%; respectively, relative risk, 1.2; 95% CI, 1.0 to 1.3) [24]. However, other studies found comparable rates of amenorrhea after CMF and CEF regimens [25,26,27,28]. The risk of amenorrhea rate after CEF calculated based on the eight studies including 1190 breast cancer patients to be 51% after six courses at 12 months of follow-up [24,25,26,27,28,29,30,31]. In the multicentre PACS 01 trial, Berliere et al. indicated comparable amenorrhea rates between patients treated with six cycles of FEC (6FEC) vs. three cycles of FEC followed by three cycles of docetaxel (3FEC/3D) at the end of chemotherapy (93% vs. 92.8%). On the other hand, in one year period, returning premenopausal hormone levels and recovered menses were more frequent in the 3FEC/3D arm than in the 6FEC arm (respectively; 43% vs. 29%, 35.5% vs. 23.7%) [29]. Zhou et al. showed different amenorrhea rates between various chemotherapy protocols; 44.87% for the FEC and 30.30% for the TE (docetaxel-epirubicin), and 23.08% for the NE (navelbine-epirubicin). Furthermore, although significant differences were not found between the FEC and TE groups, the amenorrhea rate was significantly higher in the FEC compared to the NE regimen [30].
AnthracyclinesAnthracyclines (doxorubicin, daunorubicin, epirubicin and idarubicin) exert antineoplastic effect by inhibiting the nuclear topoisomerase-II enzyme, and promoting chromosome disentanglement. Therefore, topoisomerase-II DNA complex formation is prevented, leading to the accumulation of DNA fragments and eventual death of the cell [16]. Cell viability decreases along with mitochondrial damage and free radical formation. Gonadal effects of doxorubicin are more widely investigated using several animal models [16, 32] and two human studies [33, 34]. These studies show that doxorubicin reduces ovulation rate, blastocyst formation, and reproductive life span. It also causes damage to ovarian stroma and vascular structures by inducing toxicity to both oocyte and granulosa cells of the primordial and early growing follicles. A recent animal study on mouse ovary demonstrated that doxocycline, cisplatin and taxanes can induce the apoptosis of ovarian granulosa cells (GCs), likely resulting from excessive reactive oxygen species (ROS) production-induced oxidative damage and impaired cellular anti-oxidative capacity [35].
Anthracycline-based regimens are less detrimental to the ovaries than alkylating regimens because of the lower total dosage of cyclophosphamide. For instance, 74% of patients treated with CMF developed amenorrhea in contrast to 42% receiving AC regimen [adriamycin (doxorubicin) and cyclophosphamide] [36]. Similar results was obtained in another study, which demonstrated that amenorrhea rates in patients treated with AC and CMF regimens were 53% and 83%, respectively [37]. Hortobagyi et al. reported that no patients under 30 years of age experienced menstrual abnormalities, whereas 96% of those 40–49 years of age developed amenorrhea, which was permanent for most women over 40 but was reversible for 50% of patients under 40 years of age [38]. The subsequent studies confirmed that the AC regimen did not cause amenorrhea in patients younger than 35 during two years of follow-up [39] or caused amenorrhea only in 13% of cases younger than age 40 [40]. Kil WJ et al. studied menstrual changes in breast cancer patients under 35 years of age in a retrospective study. They found similar amenorrhea occurrences (25 (31.3%) in those treated with CMF, and 34 (42.5%) in anthracycline-based regimens (AD) (p = 0.142)) and menstruation resumed in 83.1% of patients, 80% of those treated with CMF, and 85.3% with AD. The study indicates that CMF and AD protocols have similar amenorrhea or recovery rates within 54 months of the follow-up period [41]. It appears that while the risk of permanent ovarian failure is low in anthracycline regimens compared to alkylating ones in young patients, caution should still be exercised when treatingpatients older than age 35 with AC because the risk is elevated.
TaxanesTaxanes (paclitaxel and docetaxel) exert antineoplastic effects by stabilizing mitotic spindles by attaching to tubulin within existing microtubules [42, 43]. As a result, the normal microtubule breakdown (depolymerization) during cell division is impaired. Activation of the mitotic checkpoint induces reversion to the G-phase of the cell or apoptosis. (mitotic arrest). Besides, taxanes can prevent maturation of the oocyte as they prevent depolymerization of the meiotic spindles during meiosis I and II [44]. The impact of taxanes on primordial follicle pool is unknown in human and data on mouse ovary is inconsistent [45]. Taxanes are used in combination with other chemotherapy drugs, AC (doxorubicin, cyclophosphamide), EC (epirubicin, cyclophosphamide), FAC (fluorouracil, doxorubicin, cyclophosphamide) and FEC (fluorouracil, epirubicin, cyclophosphamide). Therefore it is difficult to determine its individual gonadotoxic potential. Several studies compared the amenorrhea rates between these protocols with and without taxanes. Tham YL et al. demonstrated that the rate was higher in AC + T than AC alone regimen (64% vs. 55%) [46]. By contrast, Reh et al. found no significant difference in amenorrhea rates within six months of follow-up after chemotherapy (ACT group, 29%; AC group, 41.7%). However, within the second follow-up period (28 months after chemotherapy; mean), they found higher amenorrhea rates in the ACT patients and suggested that gonadotoxicity of paclitaxel may manifest itself at more extended follow-up periods (35.7% in the ACT group, vs. 9.1% in the AC group) [47]. Another study demostrated AC and AC + T regimens exhibited similar amenorrhea rates after two years, (66.7% vs. 73.3%, respectively) [48]. Okanami et al. monitored the long-term effects of taxane on the ovary and showed that even though the amenorrhea rates during chemotherapy are significantly higher in the anthracycline+taxane arm than in the anthracycline (93.9% vs. 73.6%, p < 0.05), persistent amenorrhea rates were similar, 24.5% vs. 11.8% (p > 0.05) after three years of follow-up. The authors concluded that patients’ age at diagnosis (≤ 35 vs. ≥36) was significantly and independently associated with chemotherapy-related amenorrhea within long-term follow-up. In addition, patients in the AC + T group had longer times to resume menstruation than in AC (342 vs. 92 days) [49]. Comparison of AC, AC + T and CMF regimens in 466 premenopausal breast cancer patients forthe likelihood of resumption of menstrual bleeding after six months of amenorrhea differed significantly by treatment protocols (P = 0.002; 68% with AC, 57% with AC + T, and 23% with CMF). Nevertheless, no significant difference was reported between the chemotherapy protocols for recovery after 12 months of amenorrhea. And after two years Patients treated with CMF mainly continued to have amenorrhea (84%), followed by AC + T and AC (68%, 58%) [39]. However, another studies did not show a significant increase in the risk of amenorrhea after the sequential addition of a taxane to standard adjuvant anthracycline-based chemotherapy compared to historic controls [50] or demonstrated that the likelihood of remaining amenorrheic was not statistically different in patients who received AC-T versus AC at 33 months of follow-up (OR, 1.59; 95% CI, 0.8–3.2) [40]. A meta-analysis of 8 studies with 2124 patients found that the adjusted OR for chemotherapy-induced amenorrhea in patients receiving taxanes vs. no-taxanes combined with anthracyclins is 1.45 (0.94–2.23), suggesting a weak correlation between taxanes and the occurrence of amenorrhea [51].
Docetaxel is a semi-synthetic analog of paclitaxel. So far several clinical studies analyzed the impact of docetaxel on ovarian function in premenopuasl women with breast cancer. The PACS01 trial showed comparable amenorrhea rates between FEC vs. 3FEC/3D (93% vs. 92.8%). However, more patients in the 3FEC/3D arm recovered menses (35.5% vs. 23.7%, p < 0.05) within one year period. The study also showed that patients under age 40 treated with taxane-containing regimens had an increased incidence of reversible amenorrhea (20.5 vs. 10.5%, P = 0.025). In contrast, the incidence of amenorrhea was high in both groups for women > 40 years of age [29]. In the BCIRG 01 trial, amenorrhea rates were lower in the FAC arm than TAC (docetaxel, doxorubicin, and cyclophosphamide) regimen (32.8% vs. 51.4%, respectively) [52]. The NSABP B-30 trial assessed the likelihood of resumption of menses according to age of the patients, which were 3.2% for women > 50 years, 10.9% for women 40–50, 45.3% for patients under 40 years of age in premenopausal women received on the AC-T regimen (doxorubicin-and-cyclophosphamide-followed-by-docetaxel) [53]. The investigators also found that those treated with tamoxifen were more likely to become amenorrheic (p = 0.003). Prolonged amenorrhea was associated with a regimen that contains doxorubicin, cyclophosphamide, and docetaxel, and was age dependent and impacted by tamoxifen use [53]. Also, a substudy of this trial with 2445 patients found significant differences in amenorrhea rates among those protocols (69.8% for AC + T, 57.7% for TAC, and 37.9% for AT (P < 0.001)) [54].
A prospective cohort study showed that the amenorrhea rates were 90.2% for the TX/AC (docetaxel and capecitabine/doxorubicin and cyclophosphamide), 73.5%, for the AC-T was and 72.1% for the FAC regimen in one year, and were 66.7%, 73.3%, and 58.9% respectively, in 3 years. In addition, multivariate analysis showed that the amenorrhea rates were significantly associated with age (P < 0.001) and taxane use (P = 0.002) in the 1-year follow-up [48].
Nafaji et al. analyzed 226 breast cancer patients and found that the risk for amenorrhea was higher in taxane based protocols (52.5%, 66.7%, and 78.7% for CMF, anthracycline, and anthracycline-taxane regimens respectively). The two most significant factors for the development of amenorrhea were anthracycline-taxane-based protocols (OR: 4.059; 95% CI: 1.6–9.8) and over 40 years of age (OR, 3.5; 95% CI, 1.9–6.6) [55]. Comparison of FEC with sequential ECT, FEC-T, and concurrent ECT regimens on 165 breast cancer patients found that regimens including taxane did not increase the rate of amenorrhea compared to FEC regimens (P.0.05 for all) [56]. Another study comparing CAF (tegafur + pirarubicin + ifosfamide) with DTC (docetaxel + pirarubicin + ifosfamide) in 164 women found that DTC carries a significantly higher risk of premature ovarian failure than the CAF regimen [57].
The Impact of Tamoxifen and Ta
Comments (0)