General data
In this study, we selected 116 patients with AMI who were admitted to our hospital between January 2018 and January 2021. They were divided into the IMH group and the non-IMH group based on the presence of IMH. There were 46 cases in the IMH group and 70 cases in the non-IMH group, including 26 males and 20 females in the IMH group, aged 52–68 years old, with an average age of (62.56 ± 4.85) years old, and 41 males and 29 females in the non-IMH group, aged 51–69 years old, with an average age of (61.33 ± 4.91) years old; all patients included in the study signed the informed consent form, and the contents of the informed consent form were read to both the patients and their families: The treatments and detections used in this study are all known safe methods in clinical practice; the collected general information and clinical data were used exclusively for study analysis and for no other purpose; and patients were instructed to promptly report any discomfort during treatment to their attending physician to determine the next treatment plan. The entire treatment and observation period lasted four weeks, and patients were instructed to inform their physician immediately of any changes in their condition. Patients were not permitted to use any other drugs or treatment methods for their condition without prior approval and were instructed to inform their physician if they did. The Medical Ethics Committee of our hospital reviewed and approved this study.
Inclusion criteria: (1) The eligible patients were selected according to the clinical diagnostic criteria of Western medicine; (2) All selected patients were diagnosed with AMI; (3) Patients over the age of 18; (4) Patients requiring direct PCI in the emergency department; (5) Patients who provided informed consent and voluntarily agreed to participate in the study.
Exclusion criteria: (1) Patients presenting with cardiogenic shock, ventricular tachycardia, or ventricular fibrillation prior to the procedure; (2) Presence of valvular heart disease or congenital heart disease; (3) Patients who underwent revascularization PCI within the previous six months; (4) Patients who have contraindications to CMR; (5) Patients with incomplete medical records and relevant imaging data; (6) Participants in other relevant studies within the previous three months; (7) Pregnant or lactating women; (8) Patients with severe mental disorders who are incapable of providing their informed consent;
Rejection criteria: (1) Patients experiencing sudden deterioration of disease during the study; (2) Patients whose other diseases affect the study results; (3) Patients encountering unforeseen circumstances that make it difficult for them to continue their participation during the study; (4) Patients who have a significant impact on other researchers during the study.
Study methods
All patients underwent CMR imaging using a Philips all-digital 3.0 Ingenia magnetic resonance system. Cine sequences were used to assess left ventricular function, delayed enhancement sequences for tissue characterization, and T2-weighted imaging sequences to evaluate IMH. Patients were positioned supine and instructed to hold their breath for 12 to 15 s before images were obtained. First, the routine multi-position SE sequence scan was performed with a slice thickness and interval of 7 mm and 2.5 mm, respectively, followed by a sequence scan that included both four-to-two-chamber and long-short axis views. The echo time and repetition time were adjusted to 1.47 ms and 2.9 ms, respectively, with an angle of 45°. Then, the data of the left ventricular short-axis view and four-chamber view of the patient were collected and processed to ensure three-dimensional imaging and the content of the left ventricular volume. Gadodiamide contrast agent (Hokuriku Pharmaceutical Co., Ltd.) was administered intravenously at a rate of 3.5 ml/s and a dose of 0.2 mmol/kg for delayed enhancement imaging. After 10 min of injection, enhanced images were obtained through rapid low-angle shot sequence scanning. Specific parameters were set as follows: T1 ranged between 255 and 355 ms, with an angle of 25°. Before contrast agent administration, holding one’s breath was required for T2 data collection, information, and spin echo images. Short-axis orientation was quantified, identifying high-signal edema areas within the myocardial infarction site, with low-signal core areas surrounded by high-signal as IMH.
Left ventricular function was assessed using cine sequences. Left ventricular volume was captured in the short-axis view using a steady-state free precession (bSSFP) sequence, covering the entire heart with a slice thickness of 7 mm to minimize differences between different image types. After cine sequence imaging, the contraction and relaxation of each chamber throughout the cardiac cycle were observed, and measurements were taken of left ventricular volume (including end-diastolic and end-systolic volumes) and left ventricular myocardial mass. Left ventricular ejection fraction (LVEF) and left ventricular myocardial mass (LVMM) were calculated to evaluate cardiac function. Left ventricular function was measured by semi-automatically marking the endocardial and epicardial borders in the short-axis view at end-diastole and end-systole. End-diastole and end-systole were defined as the maximum and minimum left ventricular cavities in the central short-axis view. Papillary muscles and epicardial fat were included as part of the ventricular cavity. According to the Simpson’s rule, the sum of the delineated slices provided left ventricular end-diastolic volume (LVEDV, ml) and left ventricular end-systolic volume (LVESV, ml). LVEF (%) = (LVEDV - LVESV) (ml) / LVEDV (ml).
Delayed enhancement imaging (late gadolinium enhancement, LGE) was performed to characterize tissue. During delayed enhancement imaging, normal myocardium does not enhance and appears hypointense because the contrast agent is cleared from the extracellular space. However, necrotic myocardium appears hyperintense due to disrupted cell membrane structure and prolonged contrast agent retention. Specifically, gadoteric acid was rapidly injected via a high-pressure injector into the antecubital vein at a dose of 0.2 ml/kg and a flow rate of 2 ml/s. Ten to fifteen minutes later, under electrocardiographic gating, images were acquired at end-expiration using an ECG-triggered inversion-recovery sequence. The flip time was adjusted to suppress normal myocardial signals to zero, providing clearer images of lesions. Two-chamber, four-chamber, and six to eight short-axis views of the left ventricle were acquired.
Infarct size (IS) was determined from delayed enhancement images. On LGE images, IS was defined as the high-signal (> 2 standard deviations) area in the left ventricular myocardium supplied by the infarct-related artery. Myocardial necrosis was qualitatively defined as subendocardial (enhanced segment range < 50% of total wall thickness) or transmural (enhanced segment range > 50%). Quantitatively, the Simpson’s rule was used: infarct mass (IM) (g) = ∑ (enhanced area) × myocardial layer thickness × myocardial density (1.05 g/ml). The percentage of infarct size (IS%) = infarct mass (g) / left ventricular mass (g) × 100%. Microvascular obstruction (MVO) was defined on LGE images as a low-signal area within a high-enhanced infarct zone. The extent of MVO was calculated using the Simpson’s method, with MVO defined as the percentage of low-enhanced mass relative to total left ventricular mass: MVO degree = (low-enhanced mass / left ventricular mass) × 100%.
T2-weighted imaging (T2WI) was performed using an ECG-triggered fast spin-echo sequence (turbo spin-echo, TSE). By leveraging differences in tissue water content, images were acquired at the same short-axis positions used for cine images and were primarily used to assess myocardial edema and intramyocardial hemorrhage.
Radiologists with 10 years of experience and graduate students conducted the analysis of the cardiac magnetic resonance imaging (CMR) images. Image measurements were conducted using customized software, MR WorkSpace 2.6.3.5. Furthermore, manual delineation of the left ventricular long-short axis view, and diastolic/systolic endocardium, and epicardium was required for CMR strain analysis. Peak cardiac strain at each stage was calculated and analyzed, including global longitudinal strain (GLS), global circumferential strain (GCS), and global radial strain (GRS). Strain parameters were measured using the long-short axis view of the heart.
The relevant myocardial staining and scoring methods for contrast agents are as follows: Grade 0: absence of myocardial imaging and absence of contrast density; Grade 1: Imaging reveals partial or a minor amount of myocardial imaging or contrast agent density; Grade 2: Imaging revealed moderate partial myocardial imaging or contrast density but significantly lower expression compared to myocardial imaging or contrast density on ipsilateral or contralateral non-infarct-related contrast, indicating myocardial partial perfusion; Grade 3: It manifests as normal myocardial imaging or contrast density, but with nearly identical expression compared to myocardial imaging or contrast density on ipsilateral or contralateral non-infarct-related contrast, indicating complete reperfusion of myocardial expression. Myocardial imaging refers to the signal intensity of myocardial tissue displayed on delayed enhancement scans, which reflects the viability of myocardial cells; Contrast density quantifies the degree of contrast agent deposition within the myocardium, directly related to low perfusion in areas of necrosis or fibrosis. Both are indirectly reflected by signal intensity in CMR and are considered equivalent indicators in this scoring system.
Observation indicators
(1)
Observe the detection of IMH and non-IMH infarction sites by CMR.
(2)
Compare the results between IMH and non-IMH myocardial conditions by CMR.
(3)
Compare the results between IMH and non-IMH cardiac indicators by CMR.
(4)
Compare the results between IMH and non-IMH cardiac indicators by echocardiography.
(5)
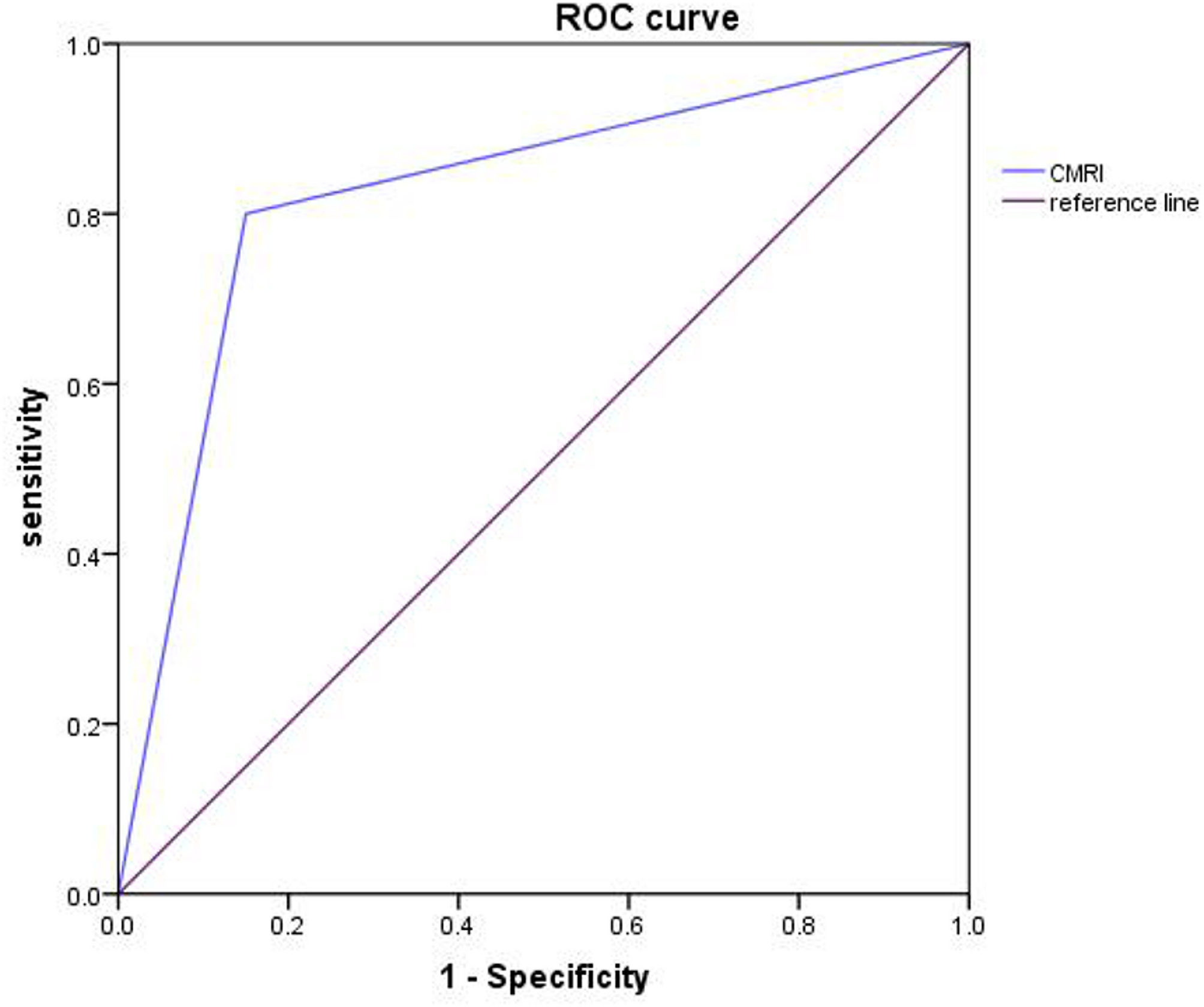
Compare the diagnostic performance of MRI in patients with AMI and intramyocardial hemorrhage by ROC curve. IMH detected by CMR was validated against a clinical composite reference standard (including peak troponin levels within 72 h post-PCI, dynamic ECG changes, and regional wall motion abnormalities on echocardiography). True positive (TP) was defined as CMR-positive IMH with clinical confirmation; false positive (FP) as CMR-positive without clinical evidence; true negative (TN) as CMR-negative without clinical IMH; false negative (FN) as CMR-negative with clinical IMH. Sensitivity and specificity were calculated as: Sensitivity = TP / (TP + FN) × 100%. Specificity = TN / (TN + FP) × 100%. ROC curves were generated using SPSS 26.0, with AUC quantifying diagnostic performance.
Statistical methods
In this research, all data were organized, and corresponding databases were established for analysis. All databases were entered into SPSS 26.0 for data processing, which included a normality test on the measurement data (expressed as mean ± standard deviation), a multi-group test conforming to normality (expressed as F), inter-group comparisons performed by t-tests, rates expressed as percentages (%), and we used the chi-squared test. ROC curves were used to compare the diagnostic performance of MRI in patients with AMI and intramyocardial hemorrhage. The difference between the datasets was statistically significant. (P < 0.05)





Comments (0)