
Remember me

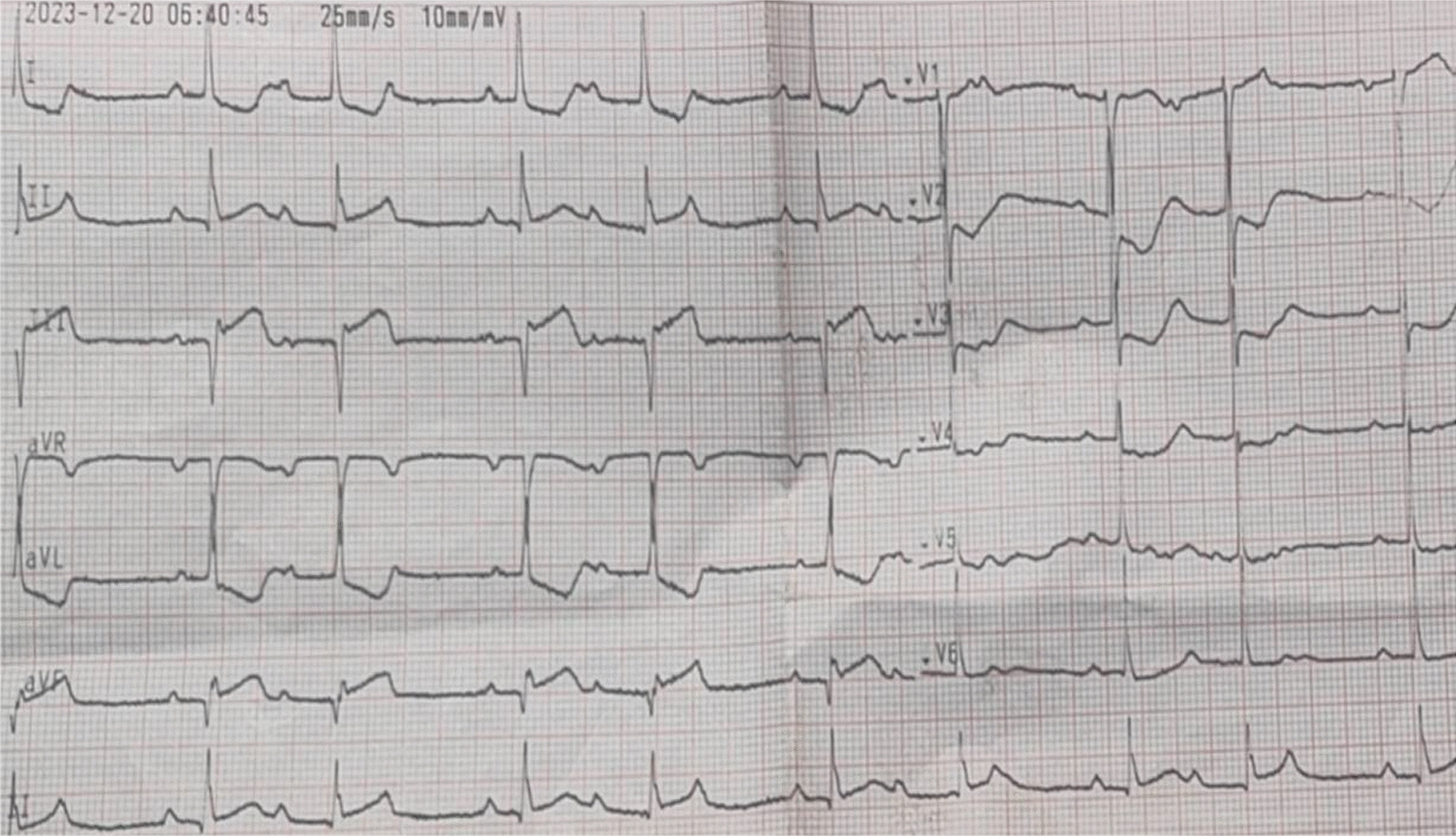



A 58-year-old male patient was admitted to a local hospital due to a 4-day chest tightness and pain, which progressively worsening over 11 h. The patient had a history of hypertension which was not previously treated, and had a history of smoking. His body temperature was 38.2 °C, his blood pressure was 116/73 mmHg, and his heart rate was 72 beats per minute. His cardiac troponin I (cTnI) level was 52.506 ng/ml, and his B-type natriuretic peptide (BNP) level was 876 pg/ml. An electrocardiogram (ECG) (Fig. 1) revealed ST-segment elevation in leads II, III, and aVF. Transthoracic echocardiography (TTE) revealed hypokinesis of the inferior wall of the left ventricle. Emergency coronary angiography (CAG) revealed 70% stenosis in the middle segment of the left anterior descending artery (LAD), diffuse lesions with 80% stenosis at the narrowest segment of the proximal to middle branches of the left circumflex branch (LCX), and complete occlusion in the proximal segment of the RCA. Percutaneous coronary intervention (PCI) was performed, and a stent (3.0*29 mm) was implanted in the middle segment of the RCA. Postoperative CAG confirmed that the RCA was patent with thrombolysis in myocardial infarction (TIMI) grade 3 blood flow. After surgery, the patient’s temperature was 36.3 °C, his blood pressure was 101/73 mmHg, and his heart rate was 76 beats per minute. A review of a Holter ECG revealed a sinus rhythm, premature ventricular and atrial contractions, an intermittent first-degree atrioventricular block, and a second-degree type I atrioventricular block. The patient was treated with aspirin and clopidogrel for dual antiplatelet therapy, statins for lipid-lowering therapy, and pantoprazole for gastroprotection. Six months after surgery, the patient’s cTnI level decreased to 0.056 ng/ml, and his BNP level decreased to 432 pg/ml.
Fig. 1
First ECG performed upon admission to the local hospital showing ST elevation in leads II, III, and aVF
Three months later, the patient was readmitted for LCX stenosis resolution. Laboratory tests revealed a cTnI level of 0.007 ng/ml and a BNP level of 389 pg/ml. ECG revealed no significant abnormalities. TTE revealed a false lumen protruding into the right ventricle around the membrane of the ventricular septum, a 6 mm defect measuring on the left ventricular side and transseptal flow shunting between the false lumen and the left ventricle. The patient was initially misdiagnosed with an aneurysm of the membranous ventricular septum with a defect. CAG was performed again and indicated that there was no more stenosis in the middle part of the RCA where the stent was implanted and that there was 60–70% stenosis in the distal segment, which was consistent with the previous CAG results. A stent (2.75*30 mm) was implanted in the LCX. On the day following the procedure, the patient reported no significant discomfort, and his vital signs were stable. He was advised to undergo follow-up TTE and further treatment at a higher-level hospital.
Four months after experiencing acute myocardial infarction (AMI), the patient came to our hospital for further treatment. The first TTE examination conducted at our hospital revealed a 6-mm rupture in the interventricular septum, with bidirectional shunting through the rupture and weakened motion of the inferior wall of the left ventricle, indicating that interventricular septum rupture (IVSR) had occurred post-AMI. Owing to the patient’s history of AMI 3 months prior and stable hemodynamics, the diagnosis was questioned by clinician. The next day, TTE examination performed by a senior sonographer at our hospital revealed a 5.0 × 4.0 cm septal false lumen at the basal part of the septum communicating with the left ventricular cavity through a 6-mm defect on the left ventricular side, and that the right ventricular septal endocardium is intact by two dimension(2D) imaging(Fig. 2a). Blood flow between the false lumen and the left ventricle was examined by color Doppler flow imaging (CDFI) (Fig. 2b and Video 1), and the shunting from the left ventricle to false lumen during systole and the false lumen to the left ventricle during diastole was examined via pulse Doppler (PW) (Fig. 2c).The movement of the inferior myocardial wall was decreased and left ventricular ejection fraction (LVEF) was 55%. IVSD occurred post -AMI was considered. Following multidisciplinary treatment (MDT), owing to the anatomical complexity and high surgical risk of repairing the interventricular septum, and the stable hemodynamics and small size of the rupture of the patient, the original medical treatment regimen continued without surgical intervention. The patient has returned to our hospital for follow-up for about 6 months, including TTE, cTnI and BNP every 1–2 months. The results revealed no significant abnormalities. Currently, the patient has no symptoms and stable hemodynamics, and the original treatment regimen continues.
Fig. 2
TTE of the parasternal short-axis view for a patient in our hospital. a 2D revealed an 6 mm-laceration in the endocardium on the left ventricular side of the interventricular septum. b CDFI revealed bidirectional shunting between the left ventricle and the false lumen through the laceration. c PW revealed that the peak systolic flow velocity at the endocardial defect of the basal segment of the posterior septum was 257 cm/s from the left ventricle to the false lumen during systole, and 163 cm/s from the false lumen to the left ventricle during diastole
Case 2A 70-year-old male patient was admitted to a local hospital due to recurrent chest tightness for more than 20 years and worsening over several hours. Emergency CAG indicated 50% stenosis in the mid-segment of the LAD, multiple 20–30% stenosis in the LCX, 40% stenosis in the proximal RCA, and complete occlusion in the mid-segment with visible large thrombus shadows. PCI was performed, and two stents were implanted in the middle segment of the RCA. Postoperatively, the patient was treated with aspirin and clopidogrel for dual antiplatelet therapy, statins for lipid-lowering therapy, and pantoprazole for gastroprotection. Upon returning to the ward, the patient experienced recurrent chest tightness and cold sweats, suggesting cardiogenic shock. Treatments, including antishock measures, vasopressors, and continuous renal replacement therapy (CRRT), were provided to reduce cardiac preloading. However, hemodynamic instability persisted, and intra-aortic balloon counterpulsation (IABP), endotracheal intubation, invasive mechanical ventilation, and low-dose vasoactive drugs were used to maintain systemic circulation. TTE indicated IVSR secondary to MI, diminished motion of the left ventricular inferior wall, and enlargement of the right ventricle and left atrium. On the 15th day after AMI, the patient was referred to our hospital for further treatment. Since the onset of illness, the patient had been bedridden, conscious but uncooperative, and anuric. The patient’s temperature was 37.7 °C, his heart rate was 129 beats per minute, his respiration rate was 11 breaths per minute, his blood pressure was 133/85 mmHg, and his pain score was 0. His white blood cell count and cTnI, creatinine, alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were 15.70 × 109/L, 1.243 ng/L, 154 μmol/L, 65 U/L, and 48 U/L, respectively. ECG indicated acute inferior wall MI. The initial several diagnosis of the bedside TTE at our hospital was IVSD On the 22nd day after AMI, TTE revealed a 5.2 × 4.2 cm septal aneurysm, at the basal part of the septum that communicated with the left ventricular cavity by multiple lacerations (entrance) at the left ventricular surface (Fig. 3a), the widest part being approximately 1.5–2.0 cm in size. The false lumen communicated with the right ventricular cavity via multiple lacerations (exit) at the right ventricular surface (Fig. 3a and Video 2), the widest part was approximately 5–6 mm; and the peak flow velocity was approximately 2.6 m/s during systole (Fig. 3b). The patient was considered to have IVSD with rupture. Mechanical ventilation, anticoagulation with heparin sodium, anti-infection treatment with ceftazidime-avibactam, gastric protection, phlegm resolution, and fluid supplementation were provided as symptomatic supportive treatments. On the 23rd day after AMI, computed tomography angiography (CTA) of lower limb arterial revealed possible occlusion and thrombosis. Owing to the patient’s critical condition, MDT was provided at our hospital. Considering that the patient had been diagnosed with IVSD with rupture, cardiogenic shock, blood-borne infection, abnormal liver function, and lower limb thrombus, surgery was needed as soon as possible. Owing to hemodynamic instability and progressive worsening, surgery was performed on the 25th day after AMI. Intraoperative transesophageal echocardiography (TEE) revealed mitral valve prolapse with moderate regurgitation caused by minor chordae tendineae rupture, and the other results were consistent with the results of bedside TTE performed on the 22nd day after AMI (Fig. 4a, b, and Video 3). Interventricular septum repair and mitral valvuloplasty were performed via cardiopulmonary bypass under general anesthesia. Postoperative TEE revealed a high echo in the posterior interventricular septum measuring 11 mm in thickness (as shown in Fig. 4c) without any abnormal shunting signal. A septal aneurysm, measuring approximately 4.6 × 3.0 cm in size, at the posterior interventricular septum, which was smaller than that before surgery, and decreased regurgitation of the mitral and tricuspid valves were noted. Postoperative physical examination revealed that the patient’s temperature was 35.8 °C, his heart rate was 76 beats per minute, his blood pressure was 127/57 mmHg, and his blood oxygen saturation was 99%. Four days after surgery, the patient died of multiple organ failure.
Fig. 3
TTE of the parasternal short-axis view on the 22nd day after AMI. a 2D image revealed IVSD with multiple lacerations on both the left and right ventricular sides. b PW revealed the peak systolic flow velocity at one of the lacerations of the right ventricular side of the IVSD was 258 cm/s
Fig. 4
TEE of the parasternal short-axis view on the 25th day after AMI. a 2D image revealed a false lumen with multiple lacerations on both the left and right ventricular sides. b CDFI revealed the left-to-right shunting through multiple lacerations on both the left and right ventricular side of the false lumen. c 2D image revealed hyperechogenicity in the interventricular septum
Comments (0)