Cardiac tumors are uncommon [3]. The estimated incidence of primary cardiac tumors (PCTs) is approximately 0.02 percent [4]. Of these, myxomas account for 30% to 50% of cases, with 75% of them developing in the left atrium and only 10% to 20% in the right atrium [3, 5, 6]. Very rarely, they originate from the IVC or Eustachian valve. Myxomas are generally characterized by their female predominance and a typical onset between the ages of three and six decades. Reviewing the previously reported cases of myxomas arising from the IVC, we found that most patients were males with an average age of 42 years (Table 1).
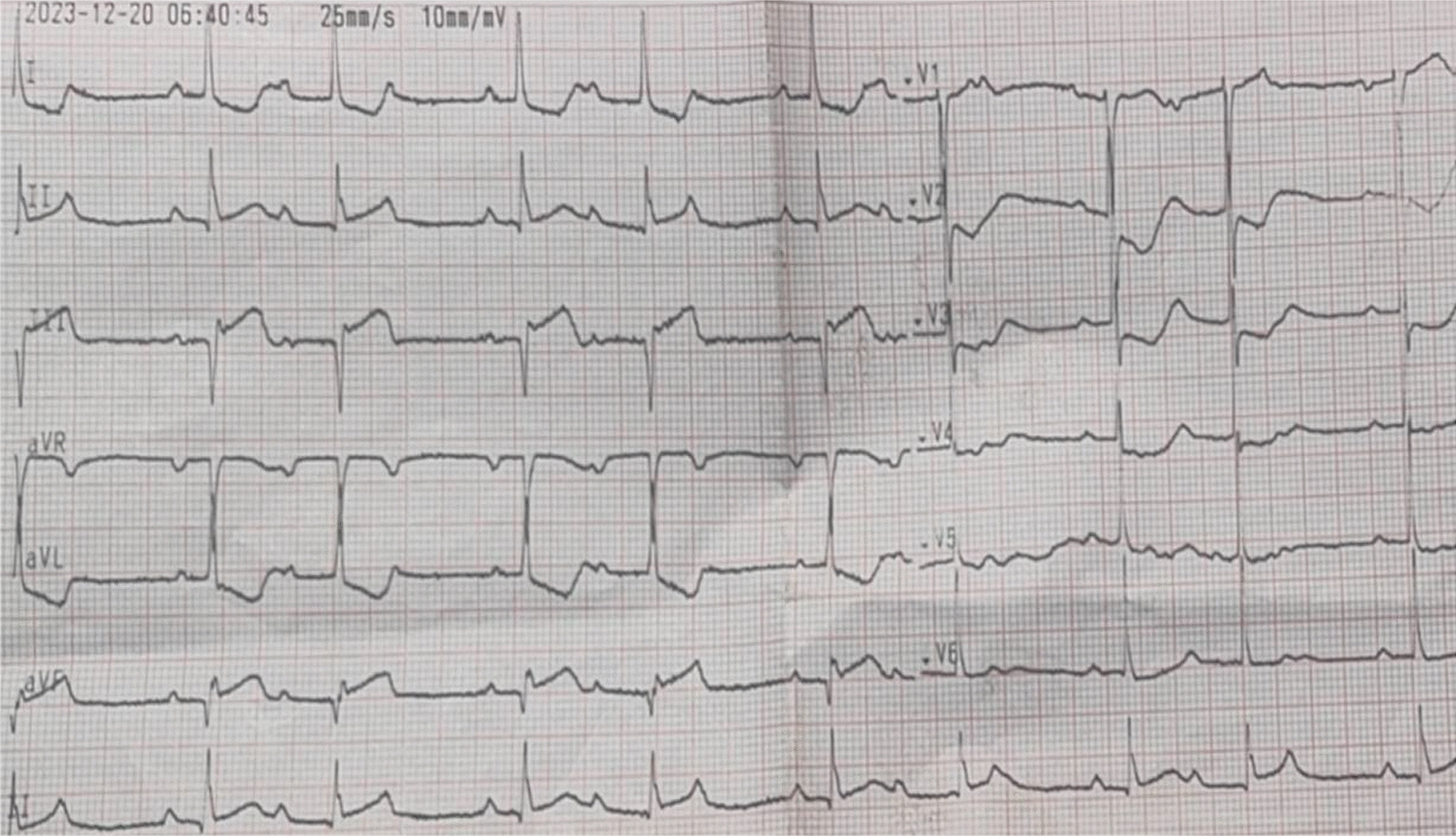
Table 1 Review of previously reported cases of myxomas arising from the IVCThe clinical presentation of myxomas arising from the IVC encompasses a spectrum of constitutional, obstructive, and embolic symptoms, influenced by factors such as tumor size, fragility, and mobility, [3, 6, 20]. Constitutional indicators, such as fatigue, fever, and dyspnea, are more common in patients with larger or recurrent tumors and may mimic rheumatic illnesses [1, 21]. Obstructive symptoms, including hepatomegaly-related abdominal distension, ascites, and peripheral edema, often manifest due to compression of surrounding structures by the tumor [22]. Additionally, embolic events can lead to symptoms such as pulmonary dyspnea and coronary angina [1, 22]. Interestingly, at least one-third of cases were found to have a murmur, while only one case was complicated by an arrhythmia (Table 1). In our presented case, the patient experienced frequent vomiting for several months, attributed to esophageal compression by the presence of myxoma in the right atrium and a displaced left atrium. Furthermore, an electrocardiogram (ECG) uniquely revealed supraventricular tachycardia (SVT), successfully managed with intravenous adenosine.
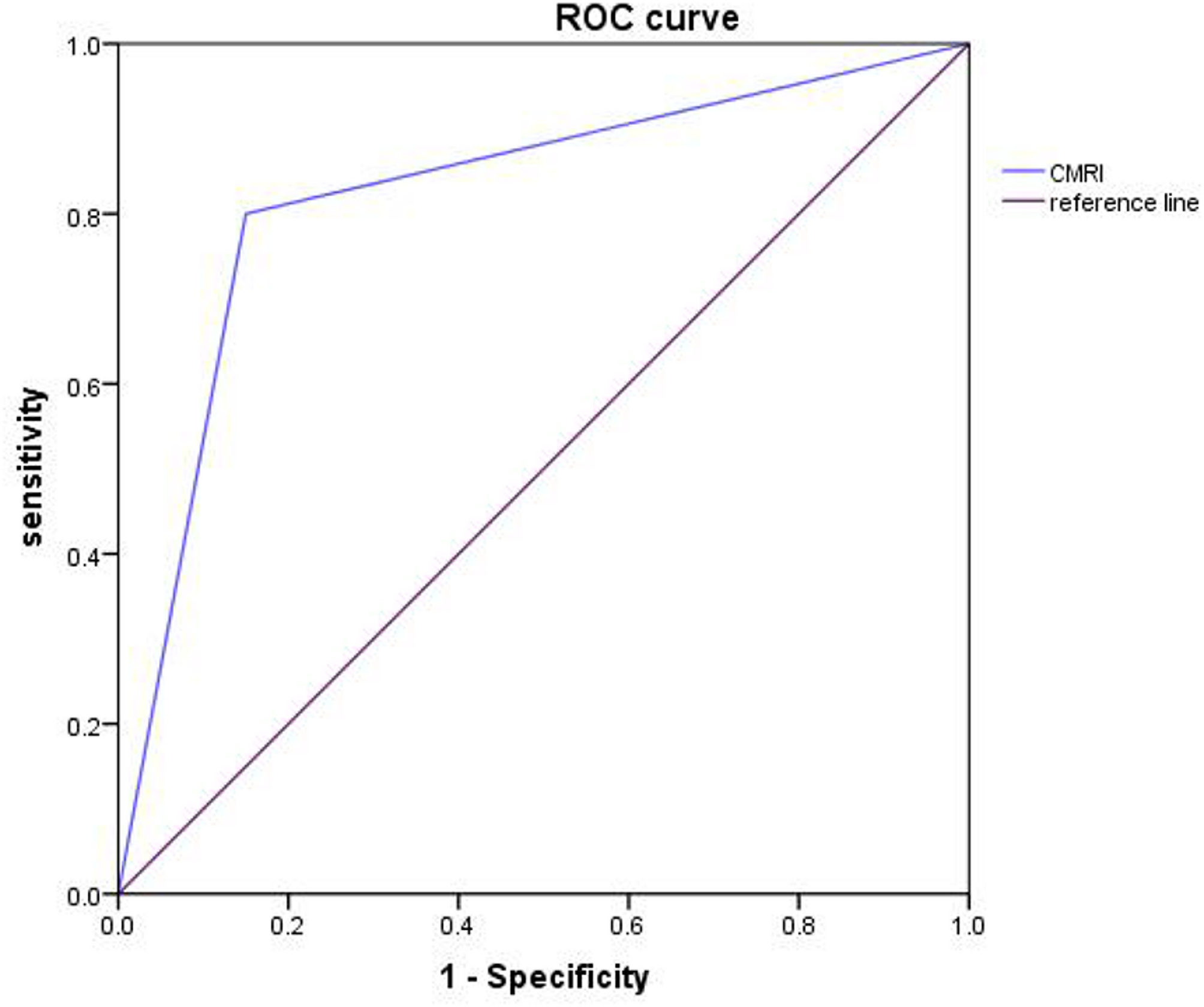
The accurate diagnosis of cardiac myxoma is significantly challenging due to its resemblance to other benign and malignant cardiac tumors, as well as various cardiovascular and infectious conditions. Furthermore, distinguishing between right atrial myxomas and right atrial thrombus can be particularly difficult. To differentiate myxomas from other masses, additional imaging modalities such as cardiac magnetic resonance imaging (CMRI) or computed tomography (CT) are often utilized to provide a more detailed characterization of the tumor [23]. CMRI allows for precise evaluation of the location and functional effects of cardiac masses across any imaging plane without exposing patients to ionizing radiation. Notably, CMRI outperforms echocardiography in characterizing cardiac lesions, helping to distinguish between myxomas and thrombi [24]. Nevertheless, echocardiography remains the primary imaging modality due to its accessibility and ability to identify specific echocardiographic features that aid in differentiation [25]. Transthoracic echocardiography (TTE) is the primary imaging tool, while transesophageal echocardiography (TEE) provides detailed localization and size assessment. Histopathological examination remains the gold standard for confirmation [9]. In this case, echocardiography identified a right atrial mass, which was confirmed as a myxoma through cardiac MRI and histopathology.
Surgical removal is considered the preferred treatment approach for myxomas. It has shown highly favorable outcomes, with operative mortality rates below 5%. The procedure is usually performed using a median sternotomy incision with the aid of CPB. Classically, venous cannulation in cardiac surgeries involving the CPB is performed using the bi-caval approach. Although most right atrial myxoma procedures were performed using this method, only one reported case used the femoral vein and SVC during cannulation, which was also the largest in terms of tumor size (Table 1). When the tumor arises from the inferior vena cava (IVC), femoral vein cannulation may be preferred to minimize the risk of embolism. This approach reduces direct manipulation of the tumor within the IVC, thereby lowering the likelihood of fragmentation and systemic embolization. The procedure mostly requires mild to moderate hypothermic arrest, however, there is only one case reported using total circulatory arrest. In our case, the right femoral vein and the SVC were cannulated and total circulatory arrest was needed to perform the resection. Excision of the main bulk of the right atrial mass was performed under 33 °C (mild hypothermia) and blood cardioplegia to protect the myocardium. Removal of the rest of the mass extending to the inferior vena cava was done using total circulatory arrest after dropping the systemic temperature to 28 °C (moderate hypothermia. The tumor measured 6 × 7 cm, making it one of the largest inferior vena cava (IVC) myxomas reported in the literature.
In most cases, surgical resection is curative, although there is a possibility of tumor recurrence, particularly in familial cases of myxomas. Therefore, follow-up is necessary with regular echocardiograms to assess cardiac function, and valvular integrity, ensure the absence of residual masses, and detect any signs of recurrence to prevent complications [26].





Comments (0)