
Remember me

One thousand two hundred and forty-six forms were submitted to the online data platform (5.1% response rate), and 1.227 (98.5%) individuals confirmed their agreement to participate. The characteristics of the responding health care professionals (95.4% physicians) are presented in Table 1.
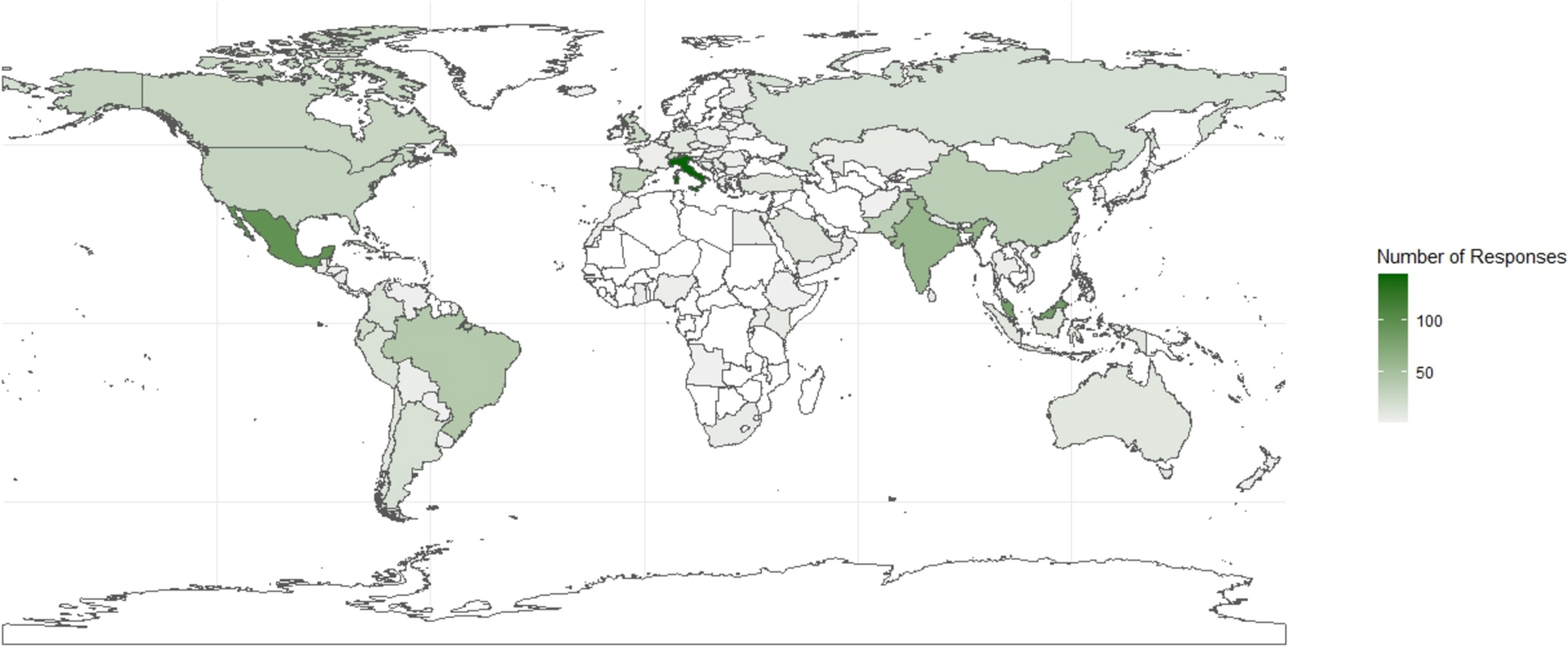
Table 1 Demographics of the 1.227 Respondents to the surveyRespondents were from the following continents: Europe (33.5%), Asia (28.3%), the Americas (30.9%), Africa (5.8%), and Oceania (1.5%). (Fig. 1) A total of 1,131 (92.2%) respondents reported inserting CVC as part of their clinical practice. The most represented specialties were critical care medicine (n:501; 27%), anesthesiology (n:407; 21.9%), and emergency medicine (n:265; 14.3%). (Fig. 2) The majority of respondents had more than six years of independent clinical practice (n:645; 51.8%) and had personally placed over 200 CVC during their medical careers (n:513; 51.3%), either independently or under supervision.
Fig. 1
Number of respondents by country
Fig. 2
Percentage of healthcare professionals responding to the survey, according to specialty
Participants reported a median US utilization rate of 70% (IQR: 40–90) for central venous catheter (CVC) insertions throughout their careers. While 12.1% consistently used US for all insertions, 6.7% relied on it for fewer than 10% of procedures, and 2.5% never used it. In the last year, a significant increase in US use was observed, with a median utilization rate of 97% (IQR: 68–100). In this same period, nearly half of respondents (46.1%) employed US for every insertion, whereas only 7.3% used it in fewer than 10% of cases.
Preferred CVC insertion siteThe preferred site for CVC insertion was the internal jugular vein (IJV) (74%), followed by the subclavian vein (SV) (17%). (Table 2) Only a minority of respondents preferred the femoral vein (FV) (6%) or peripherally inserted central catheters (PICC) (3%).
Table 2 Preferred approach for CVC positioningInsertion techniqueThe use of US was part of the standard of care for pre-insertion anatomical assessment in 54.6% of cases, for needle advancement guidance during vessel puncture in 57.2% of cases, and only in 43.8% of cases after guidewire insertion to confirm correct placement in the vein.
The preferred US technique for CVC insertion was reported to be the out-of-plane approach for IJV (63%), the FV (70%), or PICC catheters (62%). Conversely, most respondents preferred the in-plane approach for the SV cannulation (64%). (Table 3).
Table 3 Insertion TechniqueConfirmation of the appropriate CVC placement in the venous system of the upper extremitiesTo confirm that the CVC is correctly positioned in a vein (Table 4), the majority of respondents (52%) reported “always” using CXR typically in combination with other methods. The next most common technique was US visualization of the guidewire within the vein (45%), followed by saline or fluid injection (23%), observation of low-pressure blood return in the line (22%), intravascular electrocardiography (8%), blood gas analysis (6%), US contrast injection (4%), central venous pressure transduction (4%), post-insertion tip visualization via TEE (3%), and fluoroscopy (0.6%). Notably, 2.5% of respondents stated they do not routinely verify CVC positioning in the upper extremities, considering it unnecessary. Only 12% relied solely on bedside US to confirm proper CVC placement. (Table 4).
Table 4 Confirmation of appropriate placement of CVC in the venous system of the upper extremitiesTechniques to identify the position of the CVC tip at the cavo-atrial junctionAmong respondents, 5.7% indicated that they do not routinely verify the position of the CVC tip. Of the remaining 94.3%, the most commonly used method was CXR (44.9%), followed by echocardiography (24.5%), either transthoracic or transesophageal. Additional techniques included measuring the distance from the puncture site to an anatomical landmark at the cavo-atrial junction (11.4%), intravascular electrocardiography (5.6%), use of a calculated formula to estimate the required catheter length for proper tip placement (6%), and fluoroscopy (1.8%).
Among those utilizing US to visualize the catheter tip at the SVC–right atrium (RA) junction, various approaches were reported: contrast-enhanced US (using bubble detection in the RA via PoCUS or TEE) (8.2%), direct visualization of the catheter tip in the SVC-RA junction using PoCUS apical view (7.3%), or PoCUS bicaval subcostal view with confirmation via contrast medium at the exit point (6.4%). Additionally, 2.6% used TEE for direct catheter tip visualization. (Table 5).
Table 5 Techniques to identify the position of the CVC TIP at the CAVO-atrial junctionAmong practitioners using the PoCUS bicaval subcostal view (Fig. 3), 9% did not use any contrast medium, 34% used saline only, and 57% used a combination of air, blood, and saline or dedicated US contrast agents. Overall, fewer than half of respondents (44.5%) used some form of contrast medium to confirm catheter tip positioning. (Table 6).
Fig. 3
Representation of the Superior Vena Cava-to Right Atrium visualization through the trans-thoracic bicaval subcostal view
Table 6 Ultrasound contrast medium to CONFIRM CATHETER TIP LOCATIONFactors preventing the use of US as the sole method to confirm CVC placementThe main barrier to using US as the sole method for confirming CVC placement, reported by 33.9% of respondents, is the requirement to follow local institutional/departmental protocols that still mandate CXR. The second most cited concern was medico-legal liability (13.8%), followed by insufficient US proficiency (8.8%). (Table 7).
Table 7 Factors preventing the use of US as the SOLE method to CONFIRM CVC PLACEMENTRoutine methods used to exclude procedure-related pneumothoraxTo rule out procedure-related pneumothorax, 53% of respondents reported using both CXR and US, while 31% relied solely on CXR and 15% used only US. The two most frequently cited reasons for not using US exclusively to detect or exclude pneumothorax after CVC placement were institutional protocols mandating CXR and medico-legal concerns. (Table 8).
Table 8 Routine methods used to exclude a procedure-related pneumothorax and factors preventing the use of US as the only method to identify/exclude pneumothorax after placement of a CVC
Comments (0)