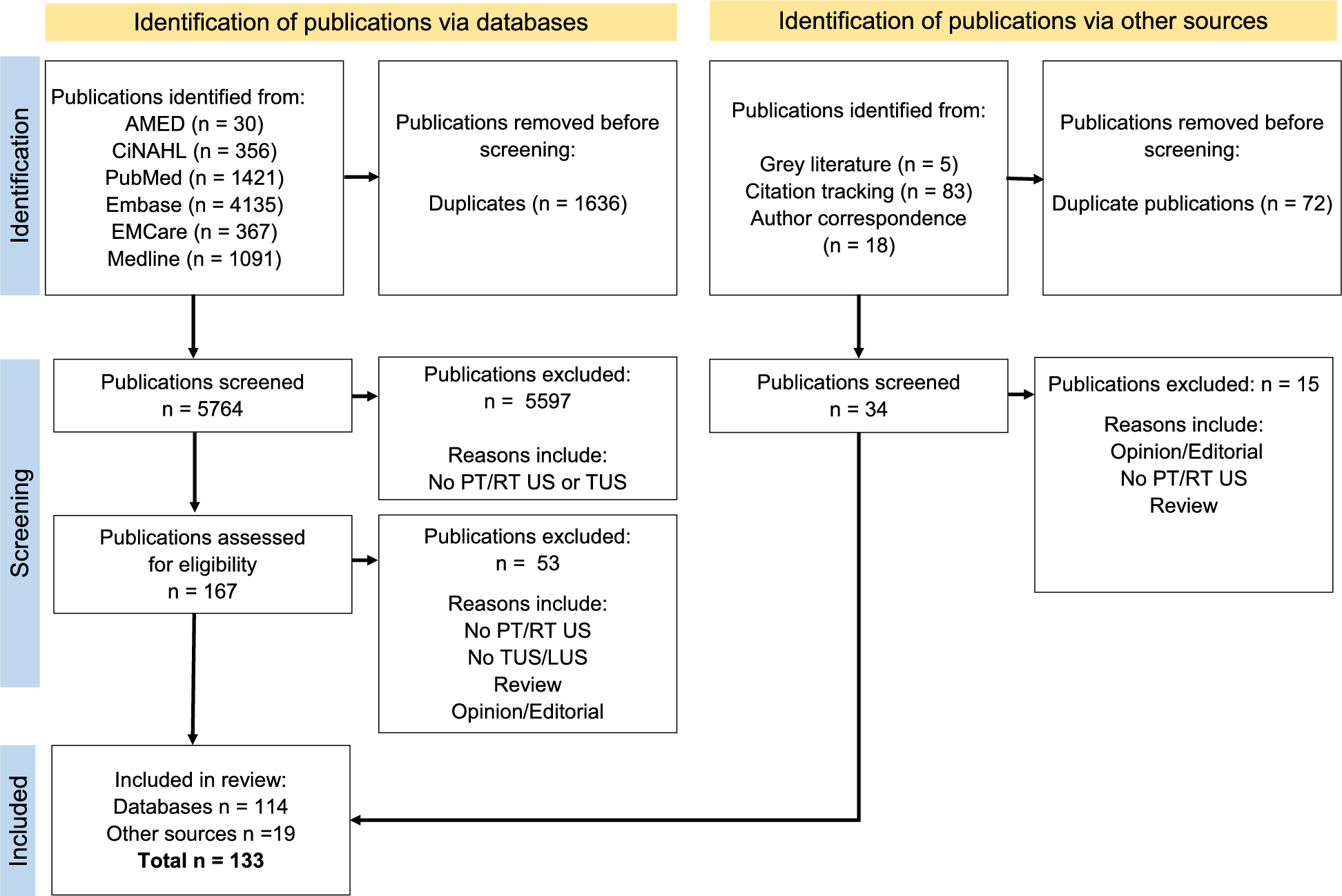
Using an enhanced search strategy, this scoping review updated the evidence around the adoption of DLUS by therapists. In the last 7 years there has been a five-fold increase in the number of studies (n = 26 to n = 133).
Geographical location
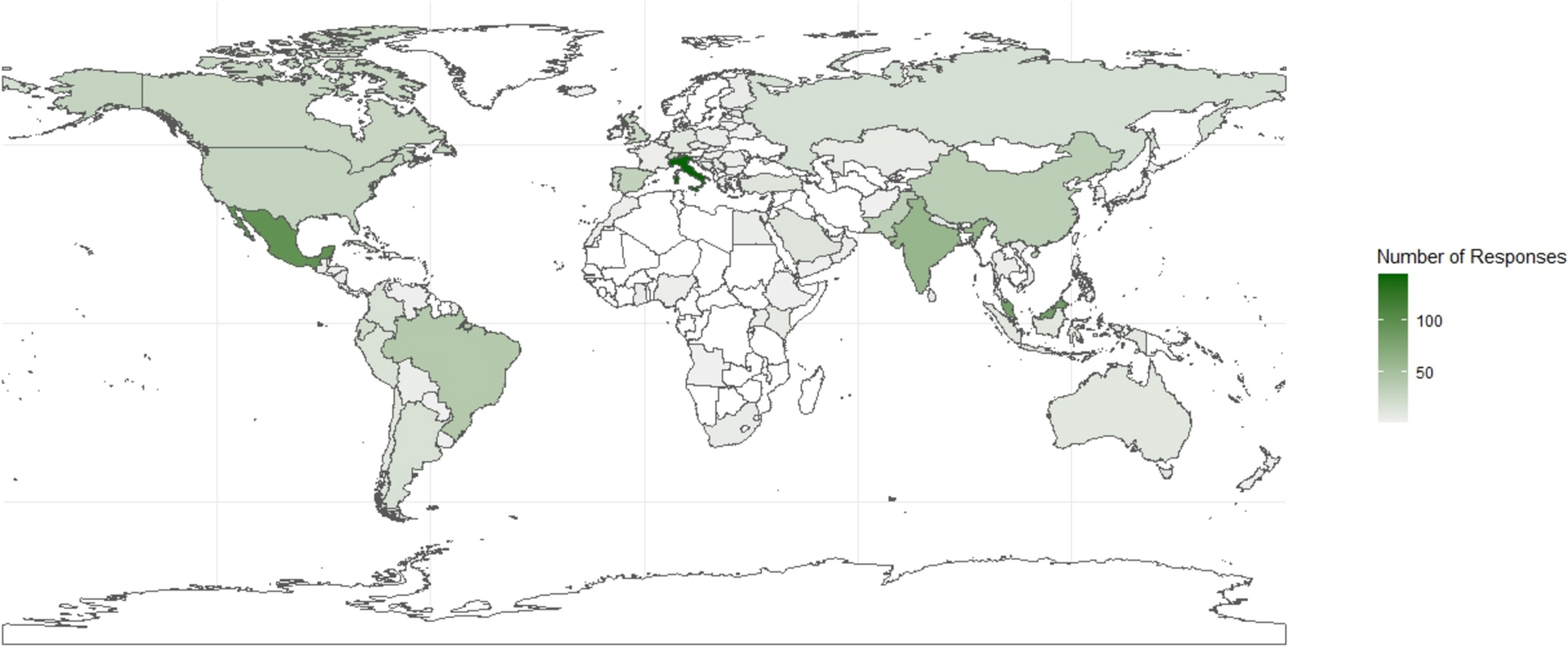
The publication of DLUS studies now has international contributions from 26 countries (Fig. 2), with the top three publishing countries (Brazil, the U.K. and Australia) being in three separate continents. The number of countries publishing therapist led DLUS research (n = 26) has almost tripled in number since the previous scoping review which included publications from 9 different countries [20]. However, all studies were published by authors from middle- or high-income countries meaning low-income countries [35] that could also benefit from the adoption of DLUS, are not represented and should be included in future work.
Participants
As with the previous scoping review [20], study participants experiencing critical illness or those with COPD represented a high proportion of the patient populations being investigated (Table 1). In contrast, the increased recruitment of healthy volunteers and therapists themselves as participants into these studies appears to suggest the development of baseline metrics regarding DLUS, and the exploration of therapist specific factors in the adoption of DLUS into practice respectively. The participant category “Patients with critical illness” includes a wide range of pathologies or conditions and would benefit from being divided into further subcategories in the future such as lung consolidation, pleural effusion or diaphragm dysfunction.
With the number of participant populations increasing from 10 to 27, the utilisation of DLUS to investigate numerous varied presentations, conditions and diseases is clearly growing.
However, less than 10% of the studies (n = 12) investigated therapists’ use of DLUS in a paediatric population. This suggests a need for additional work into this population especially considering the added safety benefits of ultrasound when compared to the ionising radiation exposure of a chest radiograph or thoracic computed tomography.
Concept
An additional 107 studies have been published between 2016 and 2023, with 35 having been published in 2023 alone (Fig. 3). This figure is more than double that of 2022 (n = 14) showing a dramatic increase in the number of research publications from therapists. Despite the number of published studies for both LUS and DUS increasing, the largest growth was seen with LUS where the number of studies went from n = 3 in 2016, to n = 58 by the end of 2023 thus showing the continued interest in this newer application of ultrasound imaging.
Even with this rapid increase of 107 studies in the last 7 years, the proportion of studies reporting that a therapist performed the ultrasound scanning themselves, has remained consistent at over 50% of the included studies (Fig. 3). This proportion could potentially be higher, but the lack of detail in reporting makes any further clarification difficult. It is recommended that both the professional background and the scanning experience of those performing the ultrasound should be included in future studies. The main point here is that as the research around DUS and LUS grows, therapists are actively participating in the performing of the ultrasound scans themselves, and not relying on other professions to perform the scans for them. This would allow therapists to perform ultrasound scans in line with the values of wider point-of-care ultrasound (POCUS) utility through therapist specific ultrasound indications, acquisition, interpretation and integration into the clinical reasoning process for enhanced patient management [36].
Context
The use of DLUS in a research capacity account for over half the included studies (52%), whether being investigated for its reliability and validity as a therapist-performed imaging tool, or as an outcome measure to investigate other treatments/interventions. Almost a third of the included studies (34%) reported on the use of DLUS as an imaging tool within clinical practice, thus highlighting the increased uptake of DLUS to enhance pathology or dysfunction identification, aid clinical reasoning towards optimal patient management, and evaluating the effectiveness of therapist’s treatments and interventions.
With the earliest search results for therapist studies in DUS and LUS having been published in 1997 and 2014 (respectively), the therapist evidence-base for DUS has been established 14-years longer than LUS. This difference is more apparent when comparing the respective included studies against the hierarchy-of-evidence [37]. Overall, DUS has a consistently higher level of evidence with most study methodologies being experimental, including 12 of the 13 RCT found (Supplementary File 1). In contrast, a large proportion of the evidence for LUS is situated lower down the hierarchy (case report/series) with fewer experimental or observational studies published (Supplementary File 1). Progress has been made in the quality of evidence for both DUS and LUS since the previous scoping review, however, focused efforts to enhance the methodological rigor of future studies, particularly for LUS, is recommended.
The high degree of heterogeneity between studies across the extracted data categories (study design, participants, disease conditions) suggests that this imaging modality remains in its infancy as all three therapist professions explore the potential adoption of DLUS within their respective research, clinical and educational practice. It is hoped that this scoping review may facilitate some degree of collaboration and coordination between these professional groups. Collaboration between the three therapy professions could benefit all, considering many aspects of research, clinical and educational practice for DLUS have some overlap.
Importantly, the higher number (n = 18) of included studies investigating education and training is encouraging (Supplementary File 1), especially alongside the emerging research outputs incorporating the governance and implementation of LUS (Supplementary File 1). In contrast, there was no published evidence around the education, adoption or implementation of DUS into therapist’s practice. The adoption of both DUS and LUS into a therapist’s practice should involve robust training processes and governance structures to guarantee high levels of therapist skill and quality assurance [34]. The framework from Smith et al. [38] in conjunction with two documents from the Chartered Society of Physiotherapists (CSP) in the U.K. on the context [39] and guidance [40] on POCUS in physiotherapy practice, may give readers the confidence to begin navigating the governance of DLUS adoption for their own practice within the healthcare systems at their geographical location.
Potential research areas
Many aspects of the use of DLUS by therapists still warrant further investigation, so listed below are some potential research gaps in the DLUS literature. Please note, this list is not exhaustive.
Financial cost versus benefit of therapist performed DLUS.
Engagement in the research and use of DLUS in low-income countries.
Additional work in the neonatal and paediatric populations.
Enhance the methodological rigor of future studies, particularly for LUS.
Additional DLUS work in respiratory interventions (i.e. inspiratory muscle training)
Expand participant populations for DUS (i.e. neuromuscular diseases)
Expand participant populations for LUS.
Robust methods of training in and adoption of DLUS needs to continue, especially as the uptake of DLUS appears to be growing internationally [1,2,3,4,5]. There is still a need to show how both DUS and LUS imaging techniques affect patient outcomes, as well as the financial cost versus benefit of therapist performed DLUS.


Comments (0)