
Remember me

This investigation was a planned secondary analysis of data from a prospective, observational study of a convenience sample of pediatric patients presenting to a level one trauma center, tertiary/quaternary ED. Enrollment was from June 12, 2022 to October 11, 2022 [12]. Appropriate Institutional Board Review was obtained.
Study protocolSelection of participantsInclusion and exclusion criteria were described previously [12]. In brief, patients aged 12 months and younger diagnosed with AB by their treating ED clinician were enrolled after obtaining written informed consent. All scans were obtained during subjects’ ED stay. Patients were excluded for immunodeficiency/immunosuppression, moderate to severe prematurity (< 34 weeks), chronic pulmonary disease, chronic moderately to severely depressed heart function based on most recent echocardiogram, sickle cell disease, chronic neuromuscular disease, or diagnosis of pneumonia within 14 days prior to ED presentation.
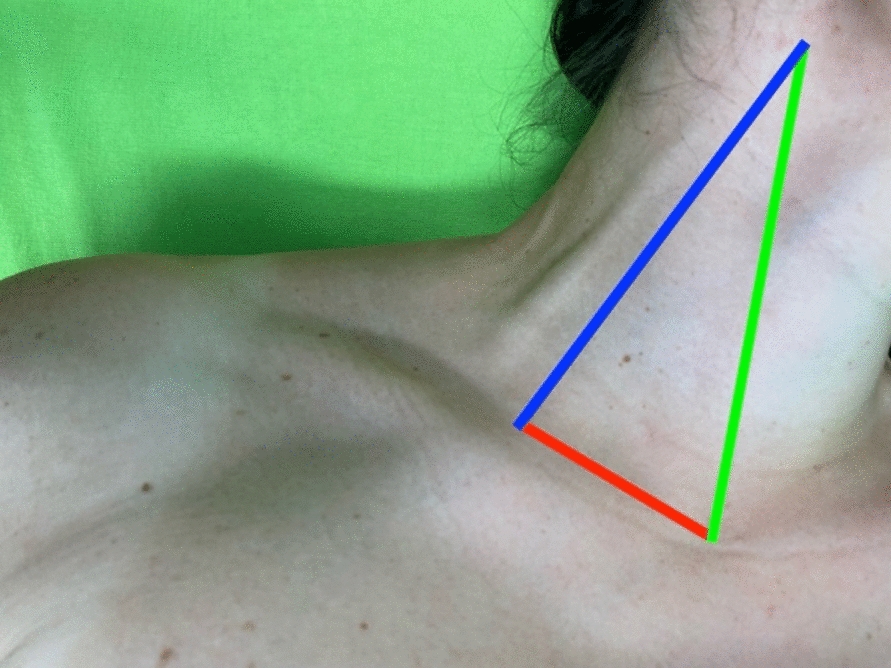
LUS techniquesThe two LUS techniques were performed sequentially. First, a “lawnmower” approach was used as described in our previous manuscript and other studies [12, 22, 28, 29] where we divided the anterior, lateral, and posterior lung fields superiorly and inferiorly for a total of 12 lung fields (Fig. 1a). Once lawnmower acquisition was complete, a posterior paravertebral “waterfall” technique was performed. The transducer was held also in a longitudinal position at the superior aspect of one of the posterior lung fields, between the medial border of the scapula and the spine. Rather than scanning side-to-side, the transducer instead was slowly dragged directly inferiorly towards the diaphragm in one motion. This process was repeated on the contralateral posterior lung field (Fig. 1b). A similar technique was described by Gori et al. [15]. Previous publications have described the posterior lung fields on LUS as most reflective of illness severity in AB [7, 13].
Fig. 1
Division of scanning fields of the lawnmower technique (1a), as previously reported.12, and side-by-side comparison of transducer movement of the waterfall technique (left) and lawnmower technique (right)
All LUS videos were obtained during the ED visit by a pediatric emergency medicine fellow who demonstrated lung ultrasound competency prior to the study [30], or one of two pediatric emergency medicine physicians with fellowship training in point-of-care ultrasound. Videos were obtained using a Sonosite X-porte with the L25 × 12–6 Hz linear transducer.
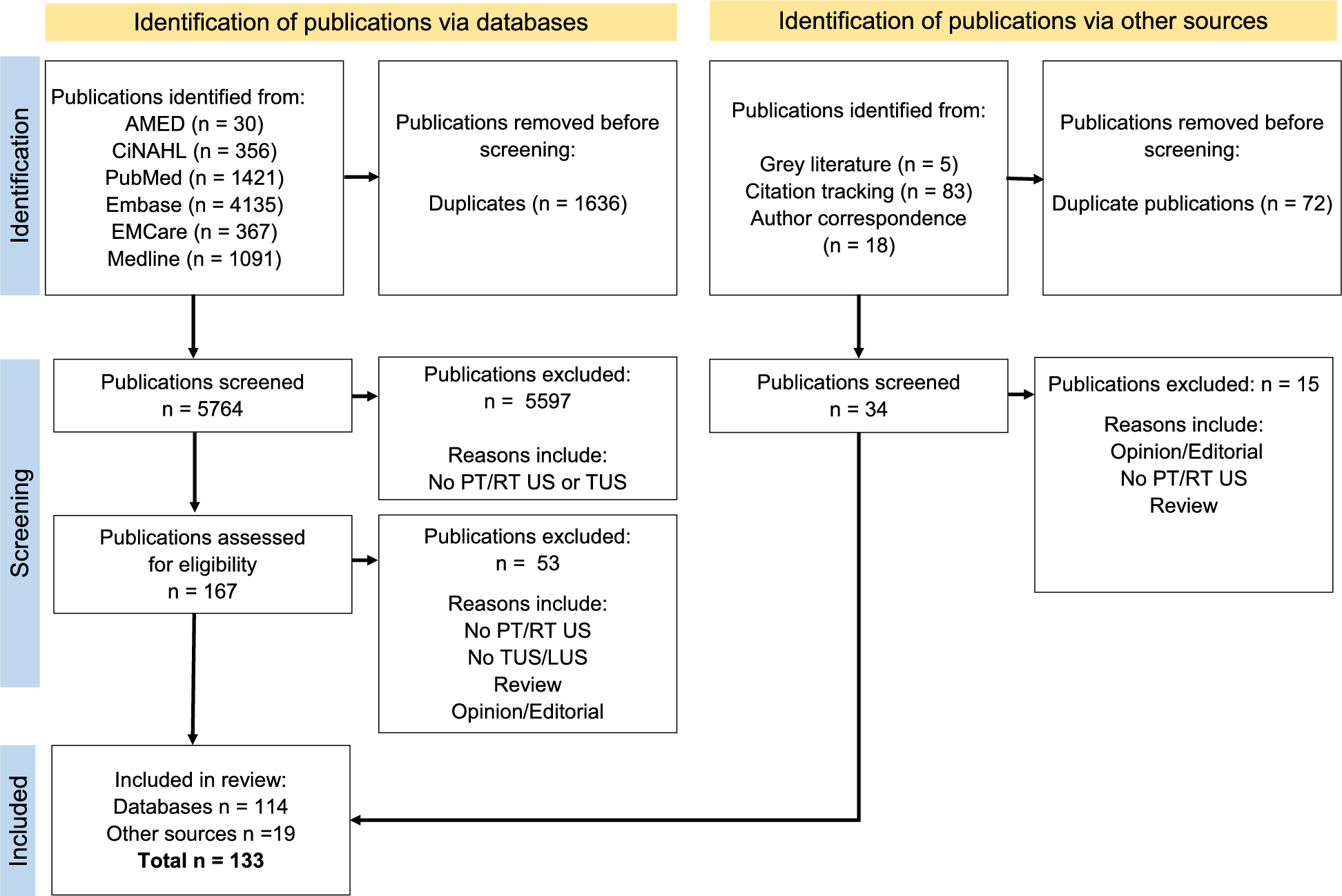
LUS scoring and documentationThe scoring for each lung field [11, 12, 29, 31] is shown in Fig. 2 and described below:
Fig. 2
- Four lung ultrasound findings. Example of the four lung ultrasound findings and associated scores, as previously reported12. (a) shows A lines (white arrows) with < 3 B lines (no B lines shown in this image), scores 0, (b) shows ≥ 3 B lines per lung segment (3 B lines shown in this image by white arrows), scores 1, (c) shows consolidated B lines, or “white out,” (white arrows) scores 2, (d) shows subpleural consolidation (shown with white *) with consolidated B lines, scores 3. In this final image, white arrows indicate air bronchograms, a common feature in subpleural consolidations
Score of 0: normal lung sliding, mostly A lines, and/or < 3 B lines per lung segment.
Score of 1: ≥ 3 B lines per lung segment, but not consolidated/ “white out”.
Score of 2: consolidated B lines/“white out,” but no subpleural consolidation or pleural effusion.
Score of 3: subpleural consolidation with any of the findings of score 1 or 2.
The total score range for the two lung fields for the waterfall technique was 0–6, and for the 12 lung fields for the lawnmower technique was 0–36. The scores were summated. Start and end times for both techniques were documented, rounded to the nearest minute, using the machine’s captured video clip times (Supplement 1).
Inter-rater reliability and quality controlWithin 30 min of completion of the LUS by the primary scanner, a second physician sonographer repeated the scan on a random convenience sample of subjects. Additionally, after patient discharge, all LUS videos were reviewed by a third physician sonographer, blinded to the original scores and patient outcomes. Inter-rater reliability (IRR) comparing the two scanners’ LUS scores, as well as comparing the post-hoc reviewer’s scoring with the scanner’s scoring, was calculated with a linearly weighted Cohen’s kappa. Rating is as follows: ± 0.81 to ± 1.00 excellent, ± 0.61 to ± 0.80 good, ± 0.41 to ± 0.60 moderate.
Chart reviewThe electronic health record was accessed for clinical data ≥ 7 days from hospital discharge. Data was manually extracted and recorded in a secure spreadsheet. These data included: patient demographics; clinical characteristics; ED findings, namely chest X-ray and respiratory viral testing results; ED disposition; and admission and discharge diagnoses. For those admitted, RS at 12 and 24 h, maximum RS during admission, and hospital LOS (measured from time of ED admission order) were recorded.
Outcome measuresWe chose the primary outcome measure as the association of the waterfall LUS score with RS at 24 h, as this seemed the most relevant to the ED clinician, but other pediatric clinicians as well. The secondary outcome was the time required to perform the waterfall and lawnmower techniques. The remainder of comparisons were exploratory and of additional interest to pediatric clinicians. These included RS at 12 h, maximum RS during hospitalization, disposition, and LOS. These are reported together with the comparison of LUS scores with RS at 24 h. Additionally, we compared these findings to the previously described lawnmower technique.
Data analysisSAS software version 9.4 (Statistical Analysis System, Cary, NC) and SPSS statistics for Windows, version 29.0.2 (IBM Corp, Armonk, NY) were used for statistical analysis. The Kolmogorov–Smirnov test was used for the normality of data distribution. Values were expressed as means ± standard deviation (SD) for continuous variables, median and interquartile range (IQR) for nonparametric data, or number and percentage (%) for categorical variables. For means, Student's t-test or Mann Whitney U test for two group comparisons and one-way analysis of variance (ANOVA) for more than two groups were used. For categorical variable comparison, chi square contingency table analysis was used. Statistical significance (p) was chosen to be 0.05 for both Pearson (normal data) or Spearman (nonparametric data) correlation coefficients.
Initial subdivisions of RS were based on institutional relevance, and included room air (RA), wall oxygen, heated high flow nasal cannula (HHFNC) < 1L/kg, HHFNC 1–2 L/kg, HHFNC > 2L/kg, non-invasive positive pressure, and invasive positive pressure (Supplement 2). Extracorporeal membrane oxygen (ECMO) and death were also considered but none captured in our data set. These subdivisions were combined into three categories for clinical relevance and generalizability: no RS (RA), low RS (wall oxygen or HHFNC < 1L/kg), and high RS (HHFNC ≥ 1L/kg, non-invasive, or invasive positive pressure).
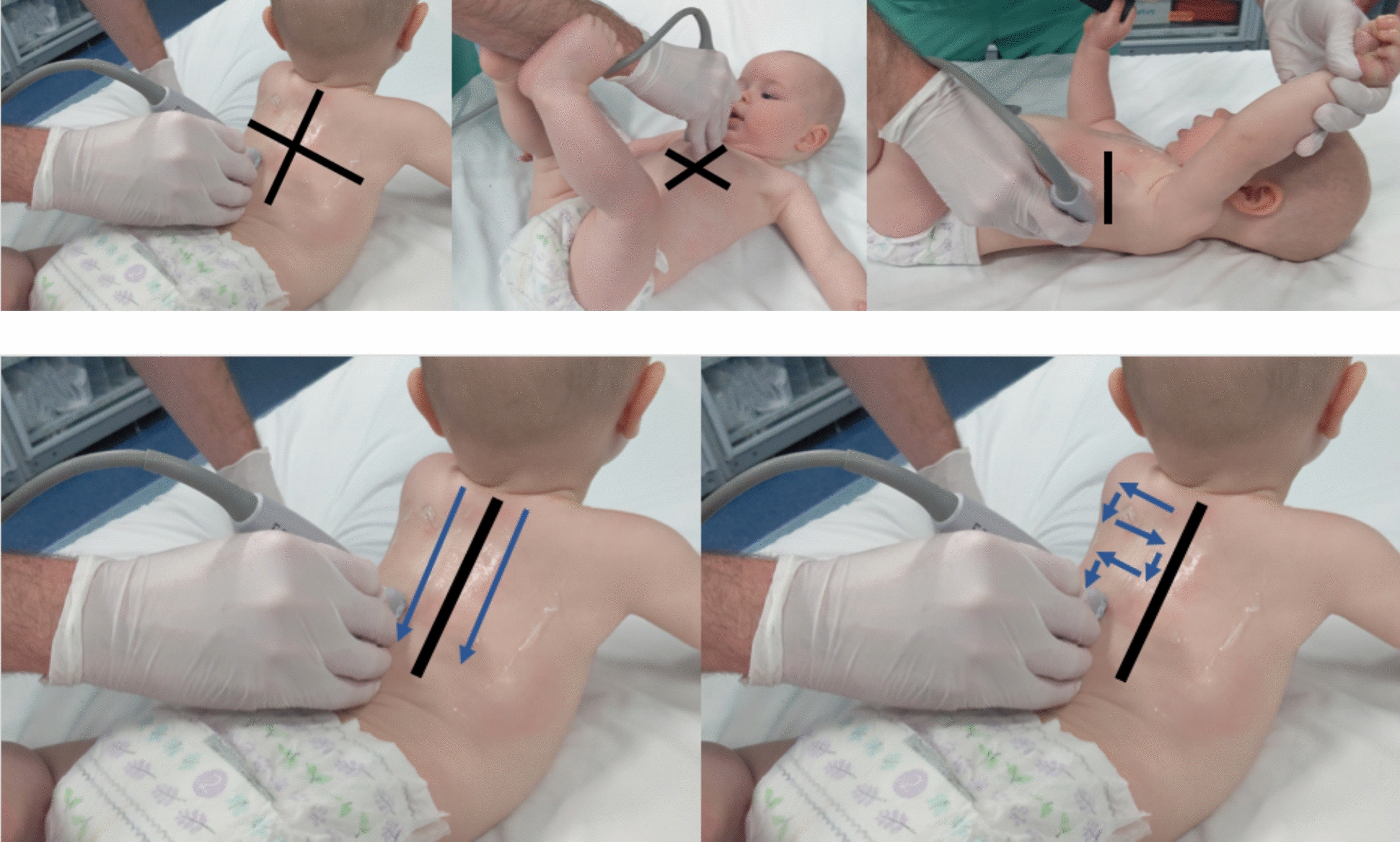
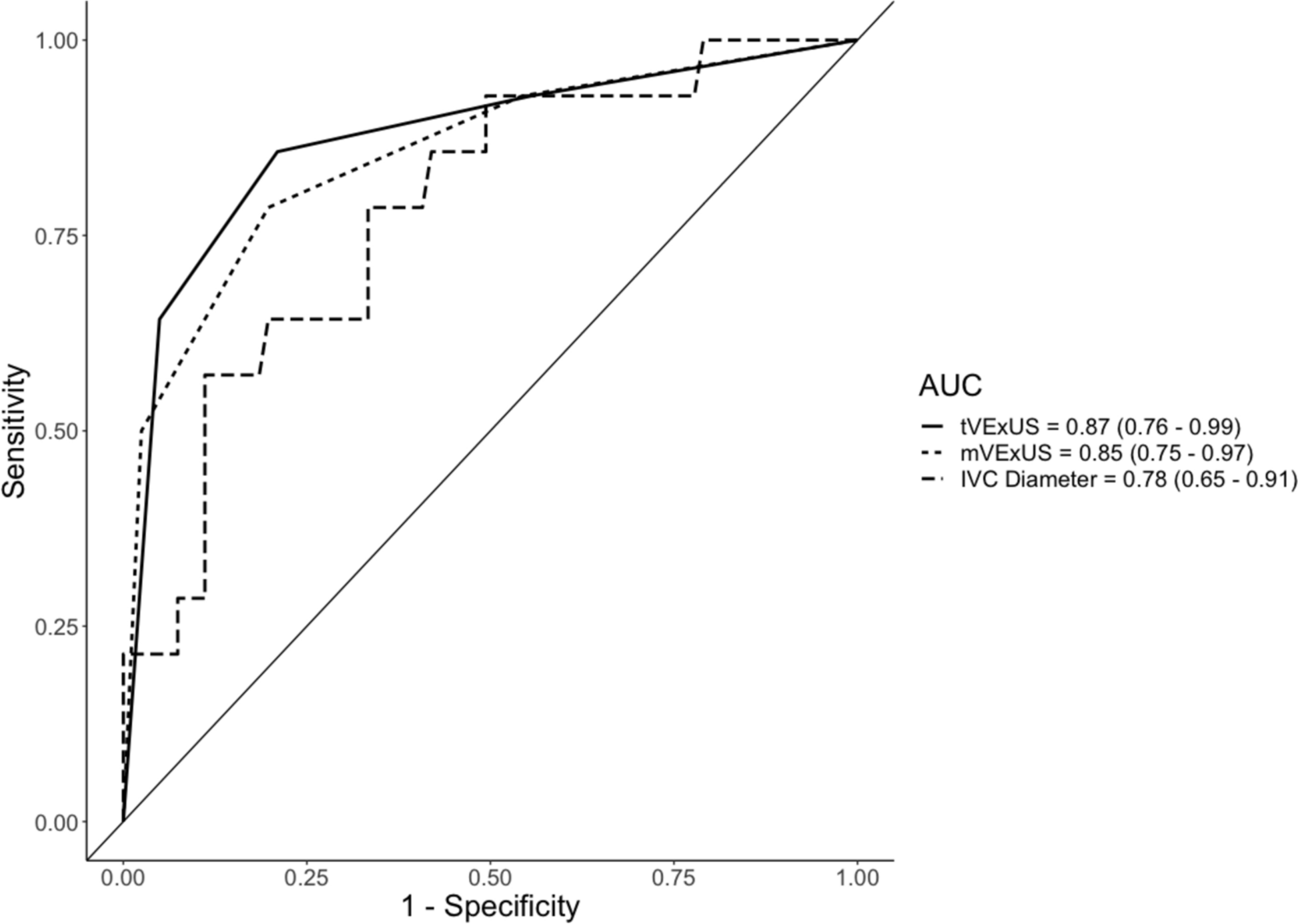
To overcome the challenge of comparing two techniques with different scoring scales (0–6 vs. 0–36), we calculated receiver operating characteristic (ROC) curves with areas under the curve (AUC), and then compared the AUCs using the Youden Index (J). This statistical tool is a function of sensitivity and specificity, and often used to measure or summarize diagnostic effectiveness, with values ranging from 0 (limited effectiveness) to 1 (very effective) [32]. Used in our analysis specifically, it allowed for comparison of the ROC curves of the two differing scoring scales. ROC curves could only be generated using binary comparisons, yet there were three levels of RS. We used integer divisions of each possible score for each technique, then compared no RS to any RS, and low RS to high RS, at 12 h, 24 h, and maximum RS, for a total of six ROC curves for RS. This was similarly done with disposition, comparing discharge and admission, as well as floor vs ICU, for a total of two ROC curves for disposition.
Comments (0)