This study has established a COS for use in future pituitary surgery research. An international modified Delphi process was used to gain consensus among key stakeholders regarding the most important outcomes to be included in the COS. The final COS includes a comprehensive list of 22 clinical and patient-centred outcomes, divided into seven key domains. It is recommended that future pituitary surgery research includes measures of these outcomes as a minimum. To our knowledge, this is the first attempt at developing a COS for pituitary surgery research.
Principal findings
The seven COS domains include: short-term surgical outcomes; nasal outcomes; ophthalmic outcomes; endocrine outcomes; quality of life and psychological outcomes; other short-term outcomes; and disease control outcomes.
While TSS for pituitary adenoma resection has undergone significant technological advancements in recent years, numerous challenges remain [21]. For example, achieving safe resection of large sellar masses invading the cavernous sinus while preserving critical neurovascular structures is difficult, often impacting the extent of resection and overall surgical outcomes [21]. Therefore, documenting surgical outcomes such as intra-operative arterial injury as well as peri-operative mortality rate—even though rare (≤ 1%), is essential, particularly as new surgical techniques are introduced into clinical practice [22, 23]. Post-operative cerebrospinal fluid (CSF) leak after TSS is a well-recognised complication, occurring in up to 5% of patients. A CSF leak has potentially serious sequelae, including meningitis, prolonged hospital stay, re-admission and need for a further operation [24, 25]. Recent innovations in surgical technology and the increasing use of artificial intelligence (AI) offer promising solutions. For example, neural networks may effectively predict CSF rhinorrhoea as well as identify key predictors [26]. With more studies assessing these outcomes, more data will become available, which could further refine predictive models to enhance risk stratification, support surgical decision-making, optimise post-operative management, and enable personalised patient counselling [26]. AI-driven early-warning systems for complications have the potential to transform post-operative pituitary surgery care. For example, high-risk patients may benefit from closer monitoring and targeted preventive measures, while low-risk patients could be considered for earlier discharge, potentially reducing hospital-acquired infection risks [27, 28].
A significant proportion of patients experience post-operative olfactory dysfunction, which is more commonly transient but is sometimes permanent, having a profound impact on patients’ QoL [29, 30]. Olfactory dysfunction can result in anxiety, depression and social isolation, reduced appetite and an inability to detect dangerous odour signals [31,32,33]. Beyond the outcome of ‘reduced sense of smell/taste’, as incorporated in the COS other important nasal outcomes should be considered. For example, the Sinonasal Outcomes Test (SNOT) is a comprehensive tool used to evaluate sinonasal morbidity, which includes additional outcomes such as nasal congestion, discharge, impaired sleep function. Studies have demonstrated it is an excellent method for assessing sinonasal quality of life by comparing pre- and post-operative results [34]. The existing evidence on olfactory dysfunction is heterogeneous and of low-level [35]. Including nasal outcomes in the COS will help ensure that post-operative olfactory dysfunction is systematically reported, monitored for and managed in future studies.
While visual deficits usually improve after pituitary surgery, a meta-analysis found that complete recovery is achieved in only 30–40% of patients, with post-operative visual deterioration occurring in up to 4% [36]. Including ophthalmic outcomes in future studies is essential for gaining a better understanding of the factors that may contribute to incomplete recovery or deterioration. Studies should systematically report formal assessments of visual acuity and fields both pre-operatively and post-operatively, essential for accurately monitoring changes in visual function [36, 37].
Endocrine outcomes are central to pituitary surgery, particularly regarding hypopituitarism recovery and management of post-operative electrolyte imbalances. Post-operative hyponatraemia occurs in 9–39% of patients, and while asymptomatic for some patients, others may require intensive care admission—increasing the morbidity associated with pituitary surgery [38]. Pituitary surgery induces new hypopituitarism in < 10% of patients, while 30% show improved pituitary function post-operatively [39]. In patients with Cushing’s disease, the risk of post-operative hypopituitarism is increased by up to 50%, particularly following repeat surgeries [40]. Additionally, the reported incidence of post-operative Arginine Vasopressin Deficiency (AVP-D), previously named Diabetes Insipidus, can be as high as 30% and approximately 2% for permanent AVP-D [39, 41]. Given its prevalence as a postoperative complication, accurately predicting transient AVP-D is crucial [42]. Incorporating such outcomes into future studies will generate more comprehensive information, facilitating comprehensive exploration of clinical factors. This, in turn, will enable HCPs to implement targeted preventive measures and personalized treatment strategies [43, 44]. The emerging use of AI also offers promising solutions such as predicting post-operative AVP-D using machine learning algorithms, demonstrating that shorter pituitary stalk, and lower pre-operative ACTH and cortisol levels were associated with a higher probability of developing AVP-D post-operatively [45].
The importance of understanding and evaluating the impact of pituitary surgery on patients’ mental wellbeing and QoL is critical yet often overlooked. Most studies have primarily focused on objective clinical outcomes, neglecting the psychological effects that pituitary surgery has on patients and their carers [46]. This gap was particularly evident in the first two Delphi rounds of the study, where patients consistently highlighted the psychological challenges they experienced and the lack of resources and support available. Patients harbouring pituitary adenomas experience psychological distress, with studies demonstrating that their QoL may not improve even after a clinically successful operation [47]. Accordingly, sexual and reproductive health symptoms—an often-underreported aspect of pituitary surgery [48]—have been incorporated into the COS. Participants frequently cited infertility, reduced libido, and sexual dysfunction, highlighting the significant impact these issues have on overall well-being and QoL. Patient-reported outcome measures (PROMs) have been tailored specifically for individuals undergoing pituitary adenoma surgery, which guided our initial list of outcomes [20]. Including QoL and psychological outcomes in the COS, as well as promoting the use and validation of PROMs, will help ensure a more comprehensive evaluation of postoperative patient wellbeing. This will facilitate a deeper understanding of the complex psychosocial challenges faced by patients, families, and caregivers throughout the treatment journey, ultimately aligning future research more closely with their perspectives.
TSS has a relatively low 30-day re-operation rate, with the most common indications being CSF leak repair, control of epistaxis and post-operative haematoma evacuation [49,50,51,52,53]. Limited data exists on the risk factors and outcomes associated with the need for re-operation for evacuation of post-operative hematoma [51]. Consequently, clinical and tumour characteristics which could predict post-operative hematoma requiring re-operation remain poorly defined. Identifying these predictors could enable stratification of high-risk patients who may benefit from closer post-operative monitoring and provide valuable outcome data to assist clinicians in pre-operative planning [54]. Re-admission within 30 days post TSS is relatively rare, with reported rates ranging from 6 to 9% and delayed hyponatremia being the leading cause [55, 56]. Recording re-admission rates and indications is a valuable key quality-of-care metric and helps identify high-risk patient populations [57, 58]. Patients with hypertension, hypothyroidism, and diabetes have a higher risk of post-operative systemic complications and re-admission [59,60,61]. However, there is limited data on 30-day re-admission rates after TSS, and predictive factors have not been clearly identified. Determining clinically relevant predictors of re-admission and understanding the typical timeframe of complications after TSS could optimise inpatient management, discharge planning, and post-operative follow-up plans, aiming to reduce preventable re-admissions [62, 63].
Recurrence for NFPAs remains high despite advancements in surgical techniques, with rates between 15–60% for those treated with surgery alone and 2–28% in patients treated with surgery and radiotherapy [64,65,66]. Additionally, many series report high rates of recurrence in functioning adenomas, such as up to 20% in Cushing’s disease [67]. Comprehensive research on clinical factors affecting recurrence rates remains limited, emphasising the need for future studies to focus on identifying prognostic factors [68]. Furthermore, the consensus process also emphasised the need for more data on additional medical therapy post-operatively. For example, while existing evidence indicates that dopamine agonists may benefit NFPA patients with residual tumour, the overall evidence remains limited [64, 69]. Additionally, remission of functioning adenomas is a key treatment goal but remains challenging to define due to the limitations of current diagnostic criteria and variability in individual responses to surgical and adjuvant therapies [70, 71]. This outcome is particularly valuable in Cushing’s disease, as it informs clinical decision-making, including whether to pursue a more aggressive surgical resection [72, 73]. Although there is demonstrated potential of machine learning (ML) algorithms in identifying risk factors and predicting recurrence and remission [74,75,76,77,78], further research is required to develop and optimise high-performing ML models for identifying clinically relevant factors. Incorporating recurrence and remission rates in future pituitary surgery studies will generate valuable data, facilitating the development of prediction models to assess treatment response and forecast recurrence risk. These innovations could improve post-operative risk assessment precision and optimise long-term management strategies.
Strengths and limitations
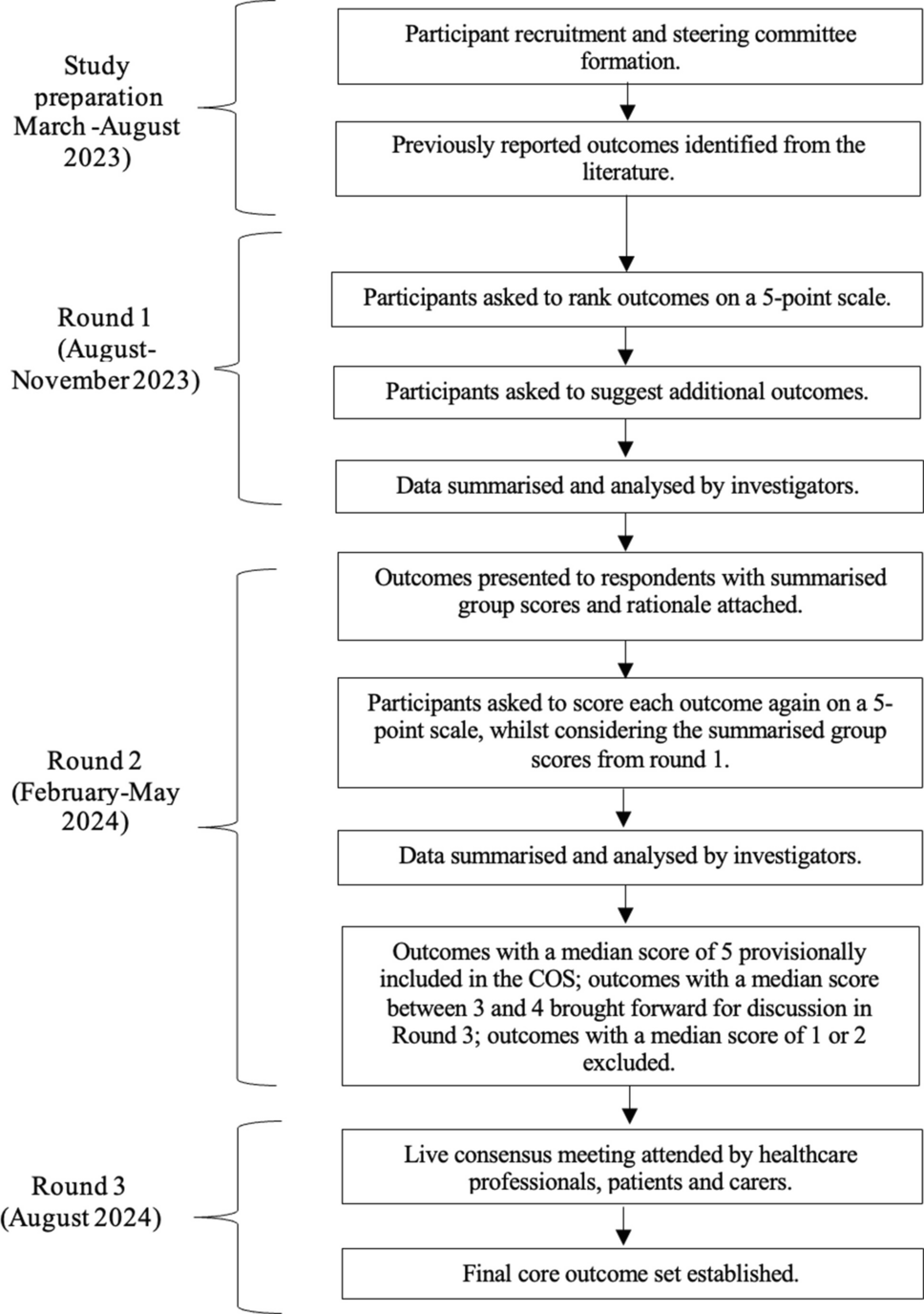
This study has several strengths. First, it was rigorously designed in accordance with the COMET Handbook and adhered to all established COS development and reporting guidelines [11, 16,17,18]. A key strength of the study is the use of the Delphi process, a well-established and validated method for gaining consensus [11]. This facilitated meaningful input from a diverse range of stakeholders, including HCPs, patients, caregivers and charity representatives. Furthermore, there was equal representation of both HCPs and patients across all three rounds of the consensus process. Active involvement of patients and caregivers is critical in ensuring their perspectives are integrated into the COS, reducing the risk of overlooking important patient-centred outcomes. Strong participant engagement and commitment was evident throughout the study. In the second round, restricted to those who completed the prior round, 87 of 95 participants (92%) continued their involvement. Additionally, user-friendly promotional materials; posters, animated videos, presentations and articles, further enhanced participant recruitment and raise study awareness. These materials were developed with guidance from public engagement specialists, ensuring that the study’s aims were effectively communicated, facilitating broad participation.
There are, however, limitations which need to be acknowledged. Despite the efforts made for international dissemination, there was underrepresentation of participants from low- and middle-income countries. Although the study had global reach, most participants were from Europe, limiting the diversity of experiences drawn from different healthcare and research systems. This lack of geographical representation can impact the comprehensiveness of the outcomes captured, as it may not fully reflect the unique challenges and perspectives of patients and healthcare providers in other settings.
Additionally, as the first two rounds of the study were conducted online, there were potential accessibility issues for individuals with limited technical literacy or visual impairment. While online surveys are efficient and accessible to many, they may unintentionally exclude certain populations.
Implications and future research
It is important to emphasise that outcomes included in a COS are the minimum outcomes that should be assessed in future research studies. However, researchers are strongly encouraged to incorporate and assess other outcomes in addition to the COS wherever possible. For example, optical coherence tomography (OCT) metrics, were included in our initial outcome list, but were excluded from the final COS, as OCT is not routinely used/readily accessible in some centres. However, where relevant, OCT metrics may be a useful outcome to record given evidence suggesting its value as a prognostic tool for post-operative visual function outcomes in some patients [79].
While the COS has defined ‘what’ to report, it is also important to establish ‘how’ these outcomes should be measured. Therefore, further work is needed to identify the best instruments and define ways to measure individual outcomes included in the COS – known as a core measurement set [80]. Additionally, next steps should include development of core data elements—a set of essential characteristics that need to be reported to facilitate the interpretation of the core outcomes.
Furthermore, given the potential bias introduced by the underrepresentation of participants from low- and middle-income countries, it would be beneficial to validate the COS in different global regions. Finally, successful implementation will require ongoing and collaborative efforts, with relevant societies adopting these outcomes. This will ensure collection of sufficient data to enable comparisons and evidence synthesis in systematic reviews and meta-analyses. Such efforts will facilitate consistent and rigorous evaluation of key outcomes, ultimately leading to meaningful conclusions that can inform the adoption of novel treatments/interventions and highlight gaps in research. It will be important to evaluate the uptake and use of this COS in standardising selection and reporting of outcomes across pituitary surgery research. This will be tracked by identifying how frequently the COS is cited as well as by conducting systematic reviews – identifying research studies which have employed it. The published COS will be shared on the study’s webpage and social media platforms as well as relevant professional and charity organisations to inform and guide pituitary surgery researchers.

Comments (0)