OSAS is a common sleep disorder. Studies have shown [13] that OSAS patients suffer from repeated breathing pauses and hypopnea at night, which leads to decreased blood oxygen saturation, thereby affecting tear secretion and tear film stability, and increasing the risk of dry eye syndrome.
In addition, OSAS patients often have changes in sleep structure, such as a decrease in rapid eye movement (REM) sleep and an increase in non-rapid eye movement (NREM) sleep. These changes can also affect tear secretion and tear film stability [14]. Studies have also found that CPAP treatment may indirectly alleviate dry eye symptoms by improving sleep quality and blood oxygen saturation [15]. In addition, the mask changes the direction of the gas, causing the airflow to be directed toward the eye above the mask. This increased airflow will also accelerate the evaporation of the tear film, causing irritation of the eye surface [16].
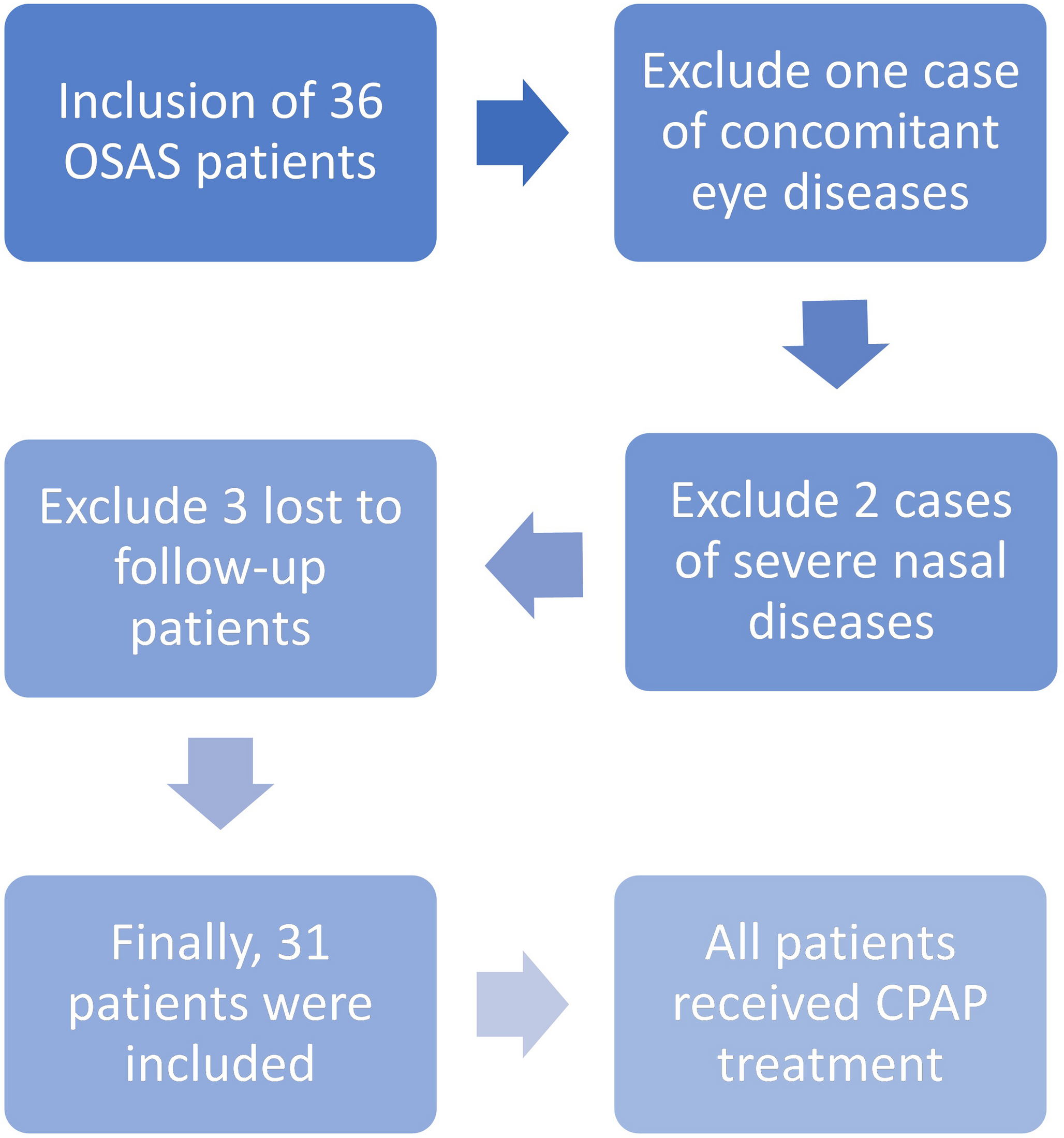
The results of this study showed that the AHI level of 31 OSAS patients after treatment was significantly lower than that before treatment, and the SpO2 levels were significantly higher than that before treatment, indicating that OSAS patients have significant clinical efficacy after CPAP treatment. The CPAP mask delivers continuous positive pressure airflow into the airway, so that the airway maintains a positive pressure state throughout the respiratory cycle, thereby treating OSAS. Furthermore, daytime hypoxemia in this study population was primarily caused by OSAS itself and was associated with persistent hypoxia resulting from nocturnal apnea events. Although BMI did not meet obesity criteria, the severity of OSAS (38.71% of patients were severe) was significantly correlated with the severity of hypoxemia, suggesting that the hypoxic characteristics of this population are directly related to the progression of OSAS rather than metabolic factors. Further analysis of the results of this study showed that the BUT time of patients after treatment was significantly higher than that before treatment. The extension of BUT time indicates that CPAP treatment can relieve dry eye syndrome, which is related to CPAP treatment improving the sleep quality of OSAS patients, alleviating hypoxia symptoms, and thus reducing systemic inflammatory response. In addition, CPAP treatment may also produce a certain positive pressure effect on the eye, promote the secretion and distribution of tears, and thus improve dry eye symptoms [17]. However, the patient’s PL score and OSDI score were worse than before treatment, indicating that CPAP treatment may cause new damage to the patient’s eyes. The possible reason is that during CPAP treatment, due to the effect of pressure, gas may overflow from the edge of the mask, and the backflow of gas continuously impacts and stimulates the ocular surface tissue. This continuous stimulation may induce ocular surface diseases such as dry eye (DE) and conjunctivitis [9, 16, 18]. In addition, the use of masks may affect blink frequency, thereby affecting the secretion of meibomian glands [19]. Frequent blinking helps the renewal of tear film and the distribution of lipid layer, while the use of CPAP masks may reduce blink frequency, thereby affecting the normal secretion and function of meibomian glands [11, 20, 21]. Once the meibomian glands are obstructed, it leads to reduced secretion of lipids on the surface of the tear film, resulting in tear film instability and rapid evaporation of moisture, ultimately causing dry eyes and potentially leading to damage or rupture of the ocular surface [22]. Therefore, the use of a CPAP mask may exacerbate meibomian gland dysfunction and further worsen dry eye symptoms. Clinically, for patients experiencing dry eye symptoms and meibomian gland dysfunction, the mask should provide adequate coverage to minimize air flow stimulation to the eyes; the part of the mask in contact with the face should be made of soft materials to reduce pressure on the meibomian glands. Additionally, the mask should feature adjustable functionalities to accommodate different facial profiles for improved comfort.
The results of this study showed that the tear meniscus height of OSAS patients after treatment was significantly lower than before treatment, while the lipid layer thickness and eye redness index were significantly higher than before treatment. The meibomian gland opening score did not change before and after treatment, indicating that CPAP treatment can improve the lipid layer thickness and eye redness index of OSAS patients, but has no effect on the meibomian gland opening score. According to existing studies [23], there are significant abnormalities in the function and morphology of meibomian glands in OSAS patients, including a high incidence of meibomian gland atrophy and morphological abnormalities, and these changes are related to the severity of OSAS. In addition, as the degree of hypoxia in OSAS patients increases, the loss of meibomian glands becomes more obvious. During the use of CPAP masks, a certain amount of airflow may be generated, which may directly or indirectly affect the eye environment and cause dry eyes. Dry eyes are an important cause of meibomian gland dysfunction, because a dry environment accelerates tear evaporation, affects the stability of the tear film, and thus has a negative impact on meibomian gland function [24, 25]. Unlike protective masks (such as N95 masks), CPAP therapy masks require high airtightness to ensure positive pressure ventilation. Their continuous use at night (average 6–8 h) and dynamic leakage characteristics (leakage volume in this study: nasal mask 10.80 ± 2.71 L/min; oronasal mask 14.72 ± 4.11 L/min) result in more sustained mechanical stimulation of the ocular surface. This unique mode of action explains why CPAP masks are more likely to cause BUT shortening and increased OSDI scores, a conclusion supported by specialized CPAP studies [11, 26]. In addition, while the mask provides positive pressure airflow, it may also exert a certain amount of pressure on the eyes. This pressure may directly affect the discharge of meibomian gland secretions, leading to meibomian gland dysfunction [27]. Physicians should choose an appropriate type and size of mask based on the patient’s specific conditions, such as the severity of the disease, meibomian gland function, and dry eye symptoms. They should also pay attention to the patient’s feedback to timely adjust mask parameters for optimal treatment effectiveness.
The results of Pearson correlation analysis showed that BUT was positively correlated with lipid layer thickness and improvement of eye redness, Sit was positively correlated with tear meniscus height, PL score was negatively correlated with tear meniscus height, and positively correlated with eye redness index. Meibomian gland dysfunction is one of the common causes of dry eye, and the morphological structure and function of meibomian glands in OSAS patients also changed significantly. Studies have shown that [28,29,30] the morphological structure of meibomian glands and the stability of tear film in OSAS patients have changed, which may be due to the decreased sleep quality and increased tear evaporation caused by OSAS. OSAS not only directly affects the stability of tear film and increases the risk of dry eye, but also further aggravates dry eye symptoms by affecting the function of meibomian glands. Therefore, OSAS patients need to pay attention to the improvement of tear film stability and meibomian gland function during treatment to reduce the occurrence and development of dry eye symptoms. Additionally, the results of this study indicate that in PSG results, AHI negatively correlated with BUT, PL scores, and OSDI scores, while SpO2 positively correlated with BUT, PL scores, and OSDI scores, but negatively correlated with the Sit score. In PSG results, AHI negatively correlated with lipid layer thickness and eye redness index, suggesting that CPAP treatment impacts dry eye symptoms and meibomian gland function, which can further influence clinical treatment outcomes. During the use of CPAP masks, leaks or gas backflow through the nasolacrimal duct can irritate the eyes and meibomian glands, increasing the risk of dry eye disease [31]. In addition, the sealing and pressure distribution of the mask may also affect the blood circulation and tear secretion of the eyes, thereby aggravating the symptoms of dry eye. Additionally, the seal quality and pressure distribution of the mask may also affect ocular blood circulation and tear secretion, further exacerbating dry eye symptoms. Therefore, in the treatment of OSAS, the choice of mask material is crucial for alleviating dry eye symptoms and improving meibomian gland function. Ideal materials should possess good breathability, comfort, and durability, while avoiding irritation to the eyes and surrounding skin. Commonly used mask materials on the market include silicone and foam. Researchers can conduct comparative analyses to select materials that minimally affect the eyes, thus reducing the occurrence of dry eye symptoms. CPAP therapy may indirectly improve BUT by alleviating hypoxia, but the design of this study aimed to elucidate the negative effects of mask-related physical factors (such as edge pressure and airflow backflow) on the ocular surface. The correlation between prolonged BUT and increased SpO₂ after treatment (r = 0.308, P < 0.05) suggests a protective effect from improved hypoxia, but the exacerbation of dry eye symptoms caused by the mask (increased PL scores and OSDI) indicates that mask-related factors play a dominant role. Although the impact of CPAP therapy on ocular surface parameters was observed, the dose–response relationship between air leakage rate and ocular symptoms was not quantitatively analyzed. Previous studies have shown that when the leakage rate exceeds 24 L/min, the incidence of ocular irritation symptoms increases significantly [11, 21]. Moreover, different mask types may have varying effects, with oronasal masks more likely than nasal masks to cause airflow disturbance in the palpebral fissure area [26]. In addition, the treatment pressure setting (8–12 cmH2O on average in this study) may have a nonlinear association with tear film evaporation rate [27, 29], warranting stratified analysis in studies with larger samples. Future research should systematically document these parameters to clarify their modulatory roles.
In summary, when OSAS patients use CPAP masks for treatment, it may have a negative impact on dry eye symptoms and meibomian gland function, leading to decreased tear film stability and aggravated symptoms such as dry eyes. This study has a relatively small sample size, and the results may have certain biases. The study period is short, and the long-term effects of mask usage on dry eye symptoms and meibomian gland function remain unclear. Insufficient comparisons among different types of masks may overlook more effective treatment options. Future research could expand the sample size and lengthen the study period to conduct a more comprehensive comparison of different types of masks, aiming to provide more effective treatment strategies for OSAS patients. Moreover, exploring other adjunctive therapies, such as pharmacological or physical treatments, could further enhance treatment efficacy.

Comments (0)