
Remember me
Ethical approval was obtained from the Institutional Review Board of the Faculty of Dentistry, Mahidol University (COA.No.MU-DT/PY-IRB 2022/061.2411). The trial was registered with the Thai Clinical Trials Registry under the number TCTR20230824001.
ParticipantsPatients were recruited from the Pediatric Sleep Clinic at Queen Sirikit National Institute of Child Health (QSNICH), Bangkok, Thailand. All patients are of Southeast Asian descent. Written informed consents were obtained prior to study participation. The following were the inclusion and exclusion criteria:
Inclusion criteria.
1.Age between 4 and 10 years.
2.Presence of signs and symptoms of POSA with AHI of ≥ 1 confirmed by type I polysomnography (PSG).
3.Friedman’s classification of tonsillar hypertrophy ≥ 2 according to an ENT evaluation [20].
4.Adenoid hypertrophy was assessed using an adenoidal-nasopharyngeal (A/N) ratio ≥ 60% (indicating significant adenoidal hypertrophy) [21].
5.Narrow and constricted maxilla with or without posterior dental crossbite according to an orthodontic evaluation.
6.Body mass index (BMI) < 25 kg/m².
Exclusion criteria.
1.Presence of craniofacial syndromes, including oral clefts.
2.Significant maxillary (overjet < -3 mm) and mandibular hypoplasia (overjet > 6 mm) in anteroposterior dimension according to cephalometric analyses [22].
3.Medical conditions contraindicated in AT.
4.History of orthodontic treatment and/or AT.
One hundred and seventy patients were screened. Of these, 130 were excluded: 115 did not meet the inclusion criteria, and 15 had contraindicated medical conditions and significant craniofacial abnormalities. Forty patients met all eligibility criteria. Among them, 16 were excluded: 1 already underwent AT, and 15 declined to participate. Finally, a total of 24 patients participated in the study.
Baseline assessment (T0)All participants underwent Type I PSG (Profusion PSG5, Compumedics, Australia) at baseline. PSG recordings were interpreted in accordance with the 2023 American Academy of Sleep Medicine guidelines [23]. Additional assessments included Friedman’s classification of tonsillar hypertrophy [20], the pediatric sleep questionnaire (PSQ) [24], and the OSA-18 questionnaire [25]. The PSQ is a validated screening tool for POSA [24]. It is also utilized to monitor therapeutic efficacy following an intervention. The OSA-18 questionnaire is a validated quality of life survey designed to measure the well-being of patients with POSA. A possible total score ranges from 18 to 126, with a higher score indicating poorer quality of life [25]. Mouth breathing was assessed through parental reports.
Dental (intercanine and intermolar widths, overjet, overbite, Angle’s classification of malocclusion) and cephalometric analyses were performed to determine baseline dentofacial characteristics of the samples. Teeth were scanned using the iTero Element scanner (Align Technology, Inc., USA) and analyzed with the OrthoCAD software (Align Technology, Inc., USA). The intermolar width was measured between the central pit of the terminal molars. Cephalometric analyses were carried out using the WebCeph (AssembleCircle Corp., Seoul, Republic of Korea). All evaluations were conducted by an orthodontic clinician blinded to patient identities and treatment groups. Both baseline and endpoint measurements were taken twice, with a two-week interval. An average of the two measurements was used for analyses. Intra-rater reliability was also calculated.
Sample size calculationThe sample size calculation was based on Marcus et al. (2013) [7]. The calculation resulted in a minimum of 10 subjects for each treatment group with 80% power to identify an AHI difference (p-value < 0.05) of 2 events/hour. Assuming a 20% attrition rate, twelve participants were required for each intervention group.
Randomization and interventionsParticipants were randomized into 2 treatment groups using block randomization with a block size of 4. They were randomly assigned to either AT or RME for treatment. The randomization was performed using Stata/SE Statistical Software, version 16.1 (Stata Corp, College Station, TX, USA).
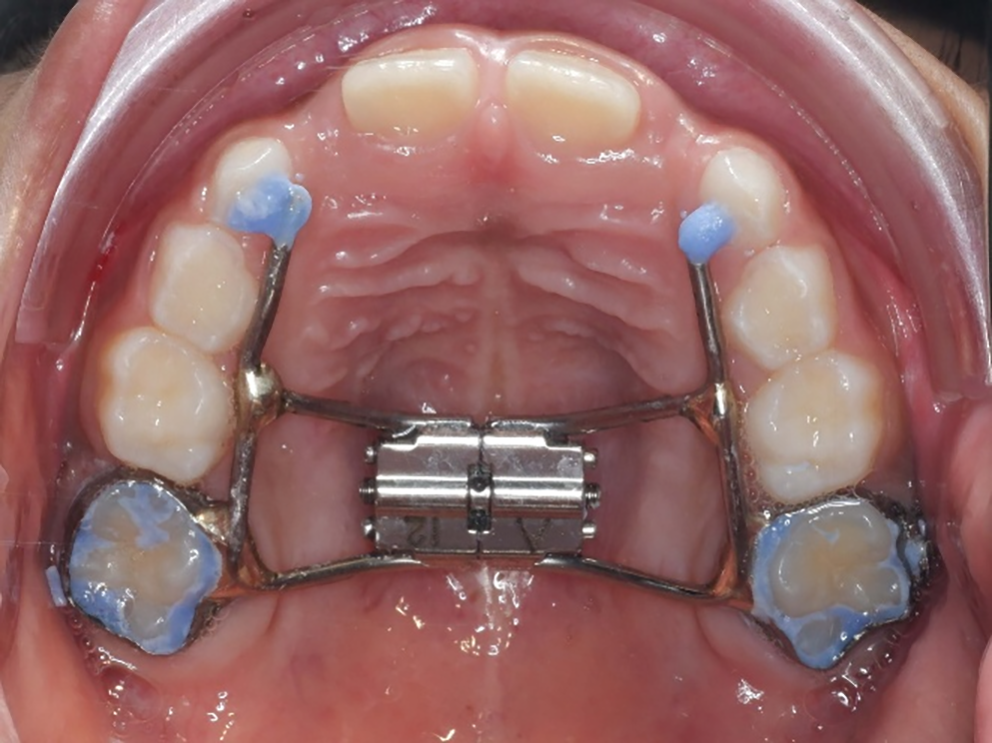
RMEThe maxillary expansion was performed by a board-certified orthodontist at the Faculty of Dentistry, Mahidol University. A dental impression was made for RME fabrication in the initial visit. RME was then fabricated in an in-house orthodontic laboratory. It utilized either the upper first permanent molars or the upper second primary molars as anchor teeth, depending on the participant’s stage of dental development. The RME featured a mid-palatal expansion screw (Hyrax, Maxi-12, Dentaurum, Germany) with arm extensions from anchor teeth to canine. (Fig. 1) It was delivered on a subsequent visit. Parents were instructed to activate the expander twice daily for 14 days (7 mm of expansion). They also received instructions on home care and oral hygiene maintenance. The device remained in place for 6 months after achieving the desired expansion to facilitate new bone formation at the mid-palatal suture. The expander was removed following this stabilization period.
Fig. 1
Rapid maxillary expansion (RME) device
AdenotonsillectomyAT was performed by a board-certified ENT surgeon following a clinical practice guideline by the American Academy of Otolaryngology-Head and Neck Surgery [3] at the surgery center, QSNICH. The surgery was performed using the extracapsular technique with monopolar electrocautery. Patients remained in the hospital for 2 nights after the surgery. They were also followed up at 7 days and 1 month by the ENT surgeon.
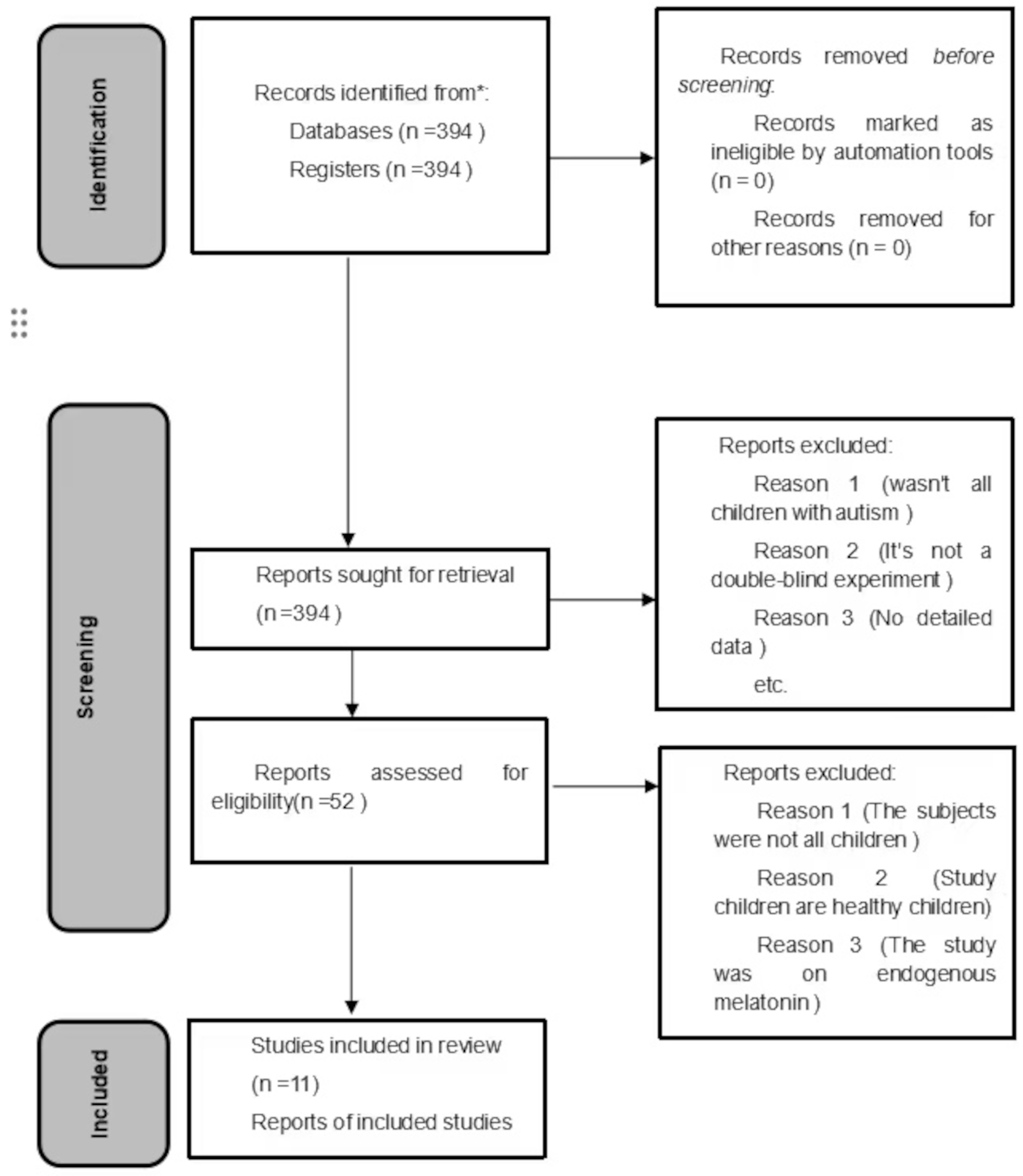
Endpoint assessment (T1)All participants underwent their assigned treatment. Follow-up assessments 6 months after treatment were performed on them. These evaluations included Type I PSG (Profusion PSG5, Compumedics, Australia), Friedman’s tonsillar hypertrophy classification [20], the PSQ [24], the OSA-18 questionnaires [25], and dental analyses (intercanine and intermolar widths). The trial flow chart is displayed in Fig. 2.
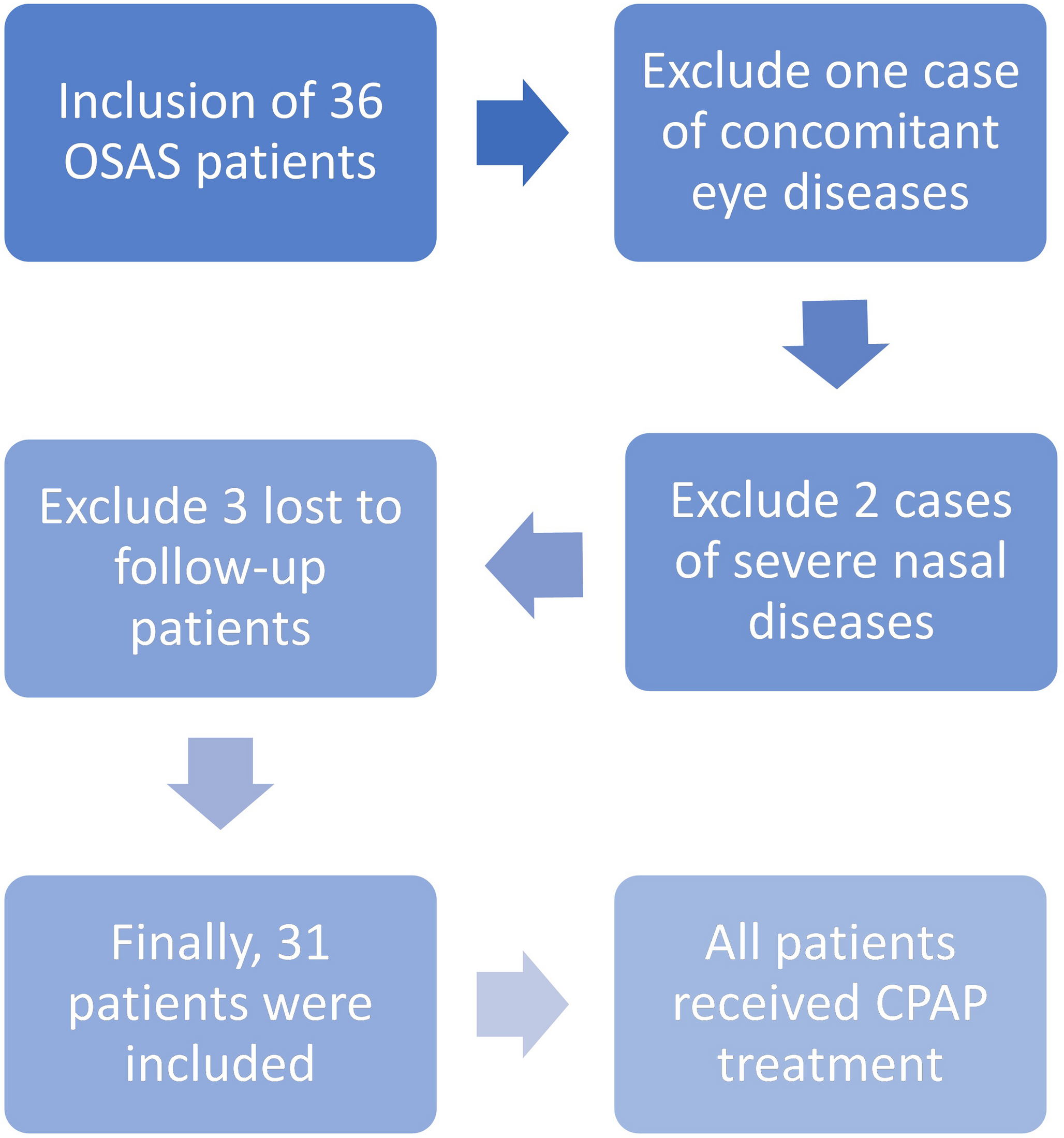
Fig. 2
Trial flow chart. Twenty-four patients with confirmed POSA, adenotonsillar hypertrophy, and constricted maxilla, were recruited for the trial. They were assigned to either AT or RME for treatment using block randomization of 4. Baseline and 6-month assessments included PSG, Friedman’s classification, dental analysis, PSQ, and OSA-18 questionnaire
Statistical analysesData distribution analysis was carried out using the Shapiro-Wilk test. For baseline and endpoint comparisons between the 2 intervention groups, independent t-tests were performed for variables that followed normal distribution (age, BMI, REM sleep time, PSQ score, OSA-18 score, overjet, overbite, intercanine width, SNA, SNB, MPA, NS-MP, MP-hyoid, facial index, and adenoidal-nasopharyngeal ratio). Mann-Whitney U tests were calculated for variables with non-normal distributions (AHI, MSAT, LSAT, intermolar width, and ANB). Categorical data (sex, Friedman’s classification, mouth breathing, Angle’s classification, and cure rate) were reported as percentages (%), and comparisons between groups were performed utilizing either the chi-square test or Fisher’s exact test.
For pre- and post-treatment comparisons within each treatment group, paired-t tests were calculated for variables with a normal distribution (REM sleep time, PSQ score, OSA-18 score, and intercanine width). Wilcoxon signed-rank test was used for parameters not following a normal distribution (AHI, MSAT, LSAT, and intermolar width). Categorical data were analyzed using the McNemar test. Intra-rater reliability was assessed using the intraclass correlation coefficient (ICC). All statistical analyses were performed using Stata/SE Statistical Software, version 16.1 (Stata Corp, College Station, TX, USA), with a significance level set at p-value < 0.05.
Comments (0)