Effect of switching from continuous positive airway pressure to bilevel positive airway pressure on symptoms of continuous positive airway pressure-related aerophagia: an observational study part two of a two-part series
Purpose
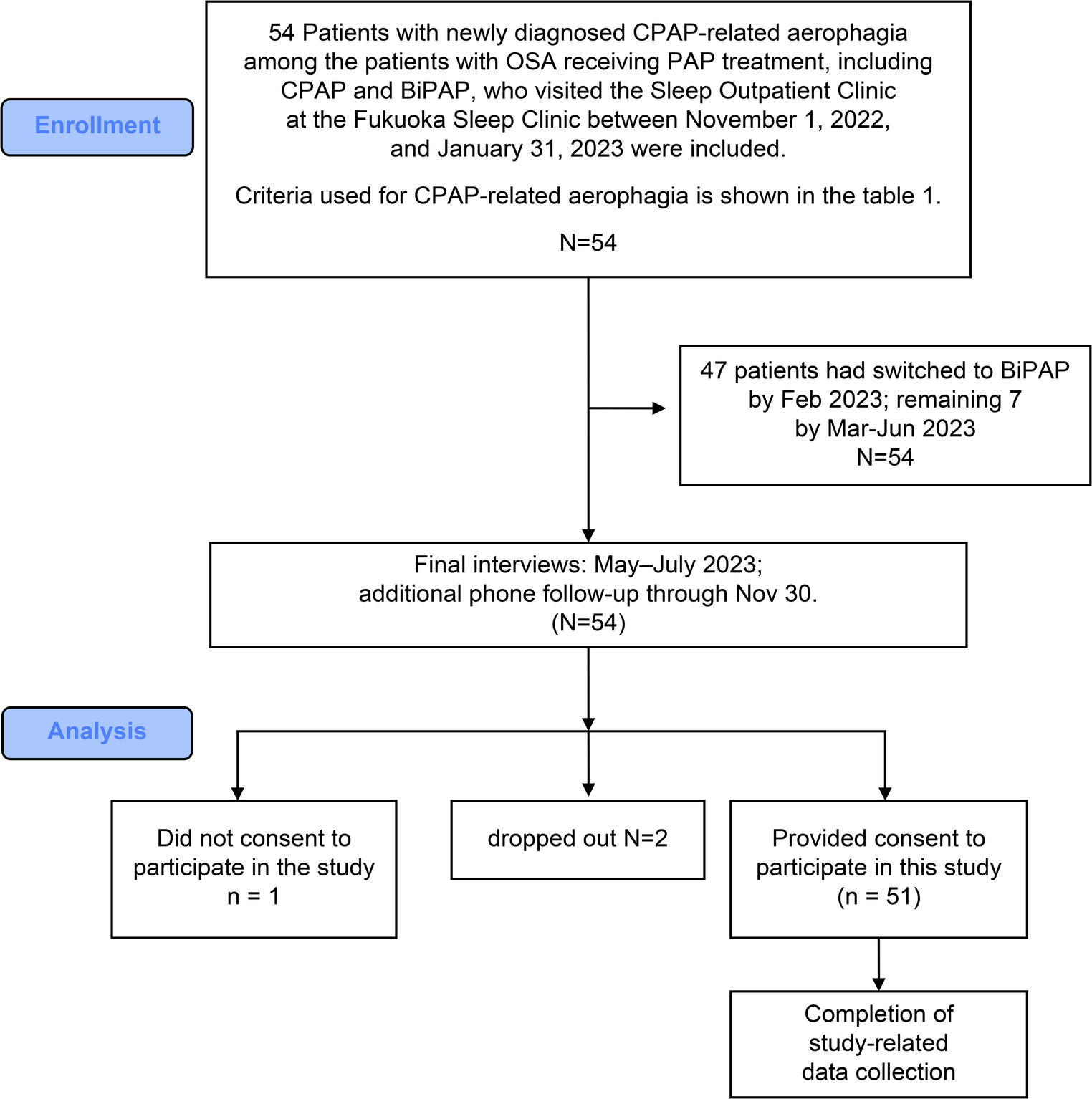
Aerophagia occurring during continuous positive airway pressure (CPAP) (C-aerophagia) in patients with obstructive sleep apnea can impede treatment. This study aimed to evaluate the use of bilevel positive airway pressure (BiPAP) for managing C-aerophagia.
Methods
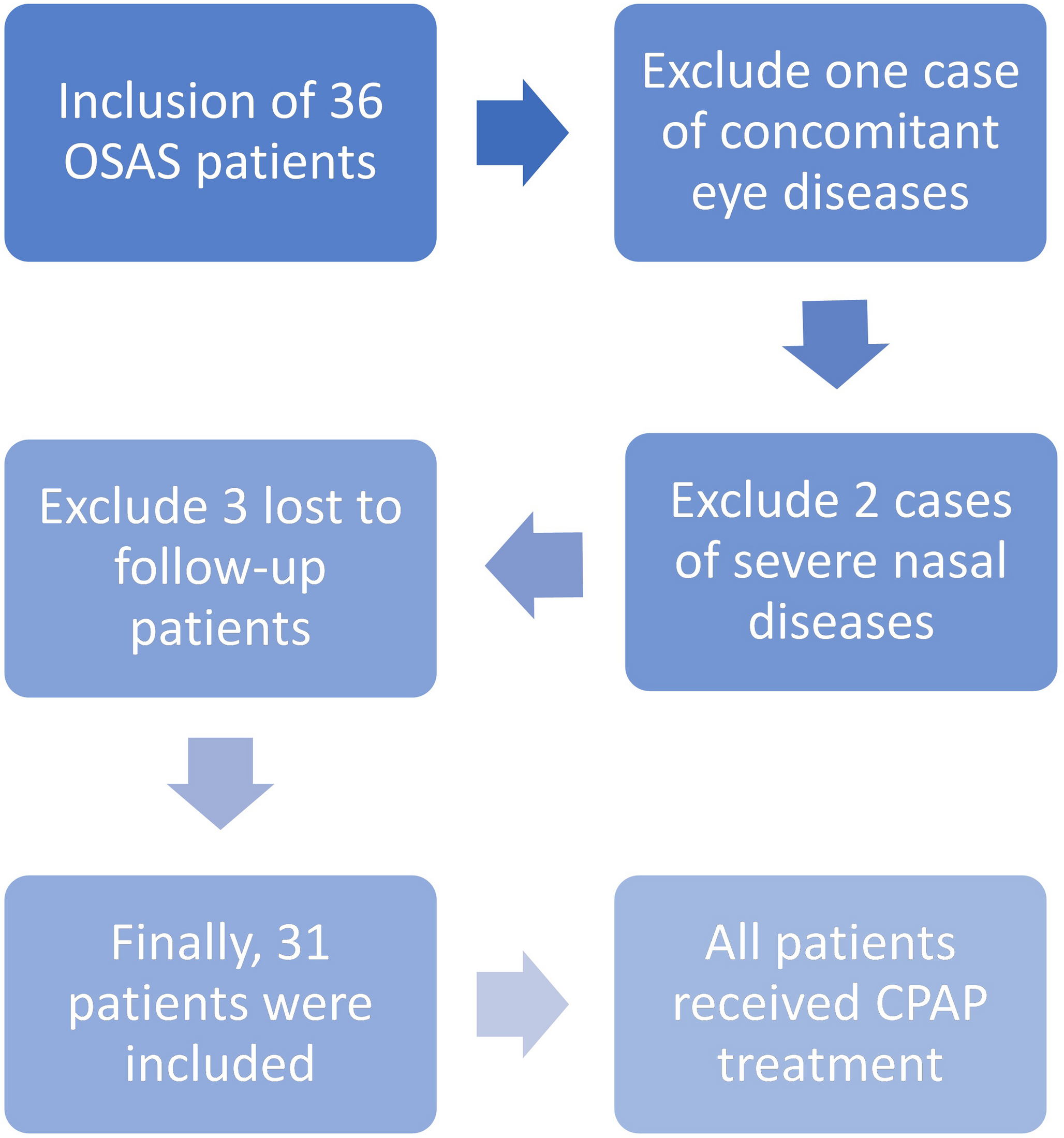
Fifty-one patients newly diagnosed with C-aerophagia who switched from CPAP to auto-BiPAP were monitored. Assessment criteria included flatulence, eructation, abdominal bloating, quantitative evaluation, and onset time. BiPAP effectiveness was categorized as excellent-E (no criteria met), slight-E (partially met), or poor-E (criteria met). C-aerophagia discomfort, including residual cases on BiPAP, was rated via a visual analog scale (VAS; 0 = none, 10 = extreme). Satisfaction with BiPAP was evaluated as positive or negative.
Results
BiPAP effectiveness was excellent in 80.4%, slight in 4.0%, and poor in 15.7% of the patients. The VAS scores decreased significantly with BiPAP compared with those with CPAP (p < 0.001). In the poor-E group, five patients reported positive satisfaction with BiPAP and showed reduced VAS scores. A reduction in 90th percentile expiratory positive airway pressure (EPAP) compared with the 90th−95th percentile pressure of CPAP was associated with resolved C-aerophagia, indicating that reducing expiratory pressure while maintaining airway patency is essential. However, eight patients with EPAP ≤ 6.5 cmH2O experienced C-aerophagia, probably due to upper esophageal sphincter relaxation, indicating that alternative treatments are needed.
Conclusion
BiPAP completely or partially resolved C-aerophagia symptoms in 84.3% of the patients. Among patients with residual symptoms, 62.5% (5/8) reported reduced discomfort and expressed satisfaction. Its effectiveness is likely due to lower expiratory pressure; however, in some cases, it remains challenging.

Comments (0)