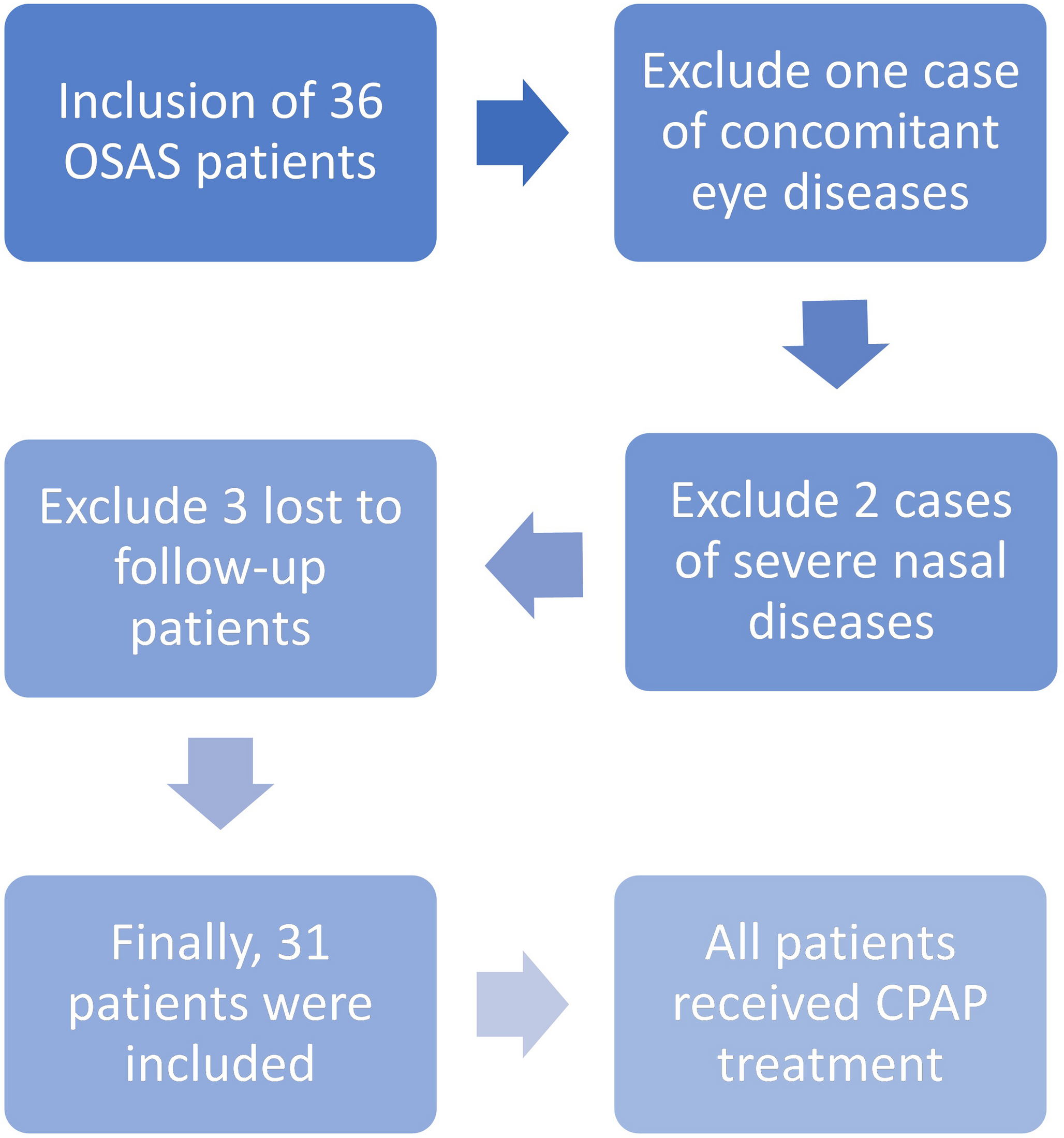
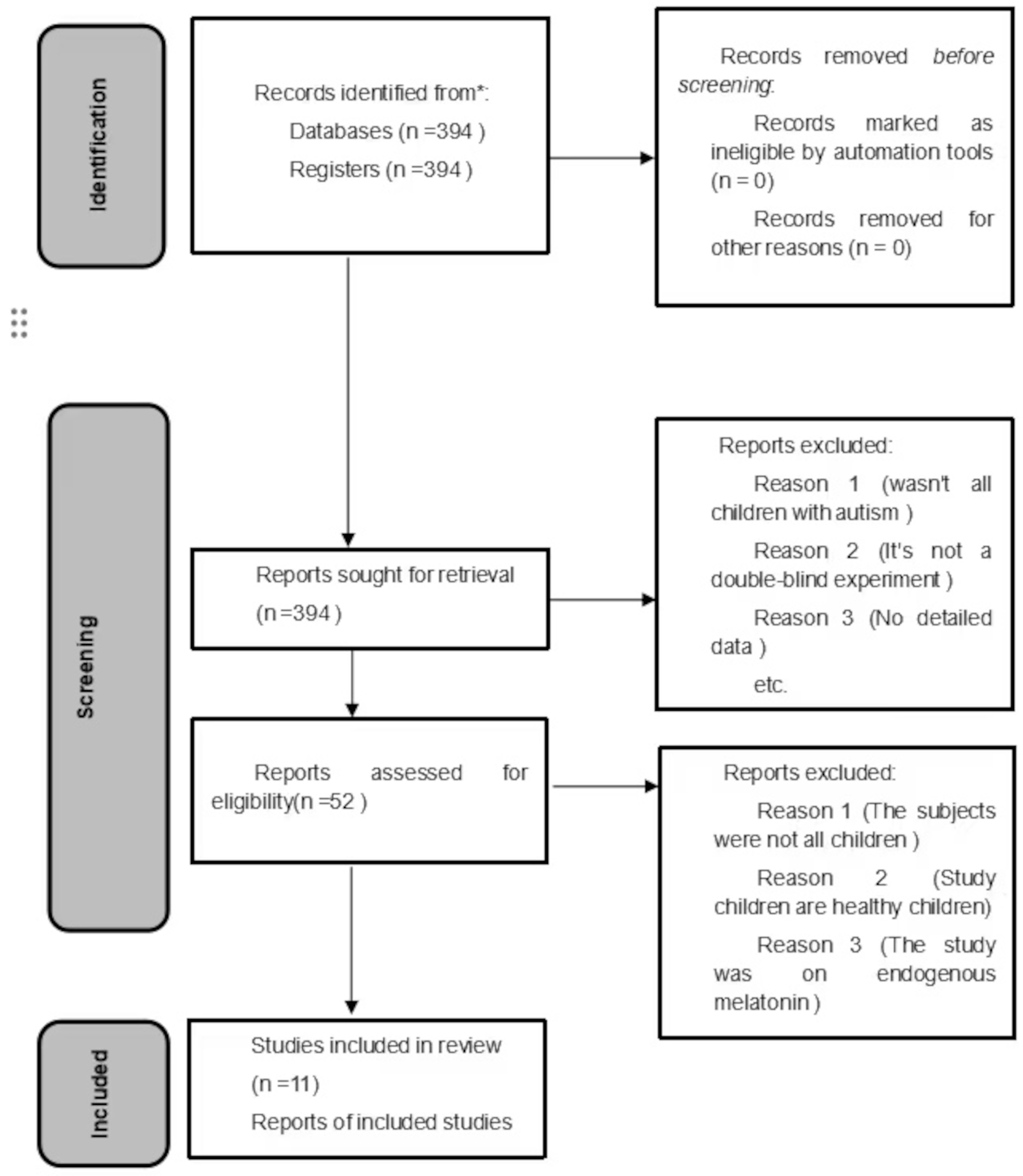
A total of 15 studies were included in the final analysis. The flowchart (Fig. 1) shows the number of studies identified, screened, assessed for eligibility, excluded (and reasons for exclusion) and included. This review included only studies with more than 1000 participants, according to the inclusion criteria, and thus most of them relied on subjective data collected via scales, questionnaires, or clinic interviews. Accordingly, of the 15 selected studies, 11 used subjective measurements (questionnaires, sleep diaries, and interviews), 1 used ICD-9 diagnosis codes. Considering the objective measurement that can be used for monitoring sleep and the sleep-wake cycle, 2 studies used actigraphy and 1 study combined actigraphy, sleep diaries, and two items of the Pittsburgh Sleep Quality Index - PSQI - “Time in bed” and “Sleep efficiency”. A brief description of study population, sleep measures and key results of the included studies are summarized in Table 1.
Table 1 Main findings of the selected studiesQuestionnaire-based studies
Subjective sleep measurements were used in eleven studies to evaluate sleep quality in cognitively healthy individuals and patients with MCI, with the main characteristics of these studies summarized in Table 2. The Jenkins Sleep Problems Scale (JSS), the Jenkins Sleep Evaluation Questionnaire (JSEQ), the PSQI were the most used tools for investigating sleep quality and disturbances, among the subjective sleep assessments. Specifically, the JSS consists of four items rated on a six-point Likert scale assessing sleep problems over the past month (not present at all = 0; present in 1–3 days = 1, 4–7 days = 2, 8–14 days = 3, 15–21 days = 4, 22–28 days = 5). The PSQI evaluates seven domains related to nocturnal sleep (sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction related to sleep problems), generating a global score that distinguishes good and poor sleepers based on a cut-off of 5. The JSEQ indicates the number of days individuals can experience problems falling asleep, staying asleep, early awakening, and awakening tired in the previous 30 days; the numbers of days were grouped according to predefined categories, and each category was given a score of 0–5, for a possible total score of 0–20.
Table 2 Main characteristics of the selected studies using subjective measurementsIn a study conducted in 2018, Suh et al. [18] analyzed a broad cohort of 2,238 participants with normal cognitive function (NC) and 655 with MCI. In NC individuals, long sleep latency (> 30 min), long sleep duration (≥ 7.95 h), and late mid-sleep time (after 3:00 am) at baseline were associated with higher risk of cognitive decline over a 4-year follow-up period. The odds ratio (OR) was 1.40 for prolonged sleep latency, 1.67 for prolonged sleep duration, and 0.61 for late mid-sleep time [18]. These associations remained significant when the sleep patterns persisted throughout the follow-up period. Conversely, among patients with MCI, by evaluating those who reverted to a NC condition, only prolonged sleep latency was associated with a lower chance of reverting to NC (OR = 0.69) [18]. In summary, sleep problems emerged as potential indicators of developing MCI in NC individuals, whereas only prolonged sleep latency resulted as a sleep problems reducing the possibility of reverting to NC in patients with MCI.
The study by Chen et al. (2016) [19] examined the association between sleep duration and risk of MCI and dementia in 7,444 women aged 65 to 80 years old. From the analysis of the study findings, a V-shaped association was observed between sleep duration and longitudinal risk of developing MCI or dementia. In particular, both short (≤ 6 h/night) and long (≥ 8 h/night) sleep durations were associated with higher risk of conversion to dementia compared to intermediate, normal, sleep time (set at 7 h per night). Specifically, short sleepers had a 36% higher risk and long sleepers - without cardiovascular disease - had a 27% higher risk of developing MCI or dementia at the longitudinal observation [19].
Expanding on the link between sleep duration and cognition, Jackowska and Cadar [20] included in their study 4,877 participants to assess the relationship between sleep duration and cognitive performance over time. Sleep duration, a measure of average self-reported number of hours of sleep on a weeknight, was categorized into four groups: “≤6 hours” and “6–7 hours” (short sleep duration), “7–8 hours” (optimal sleep duration), and “>8 hours” (long sleep duration). Among men (mean age of 65.4 ± 8.8 years), both short (≤ 6 h and 6–7 h) and long sleep durations (> 8 h) at baseline were associated with a higher risk of presenting lower scores on verbal memory tests at the 8-year follow-up, particularly in delayed recall test. Conversely, the group of male subjects with optimal sleep duration (7–8 h per night) did not present this risk (total effect: β = −0.263, C.I. −0.506 to − 0.020). No significant associations were observed between sleep measures and cognitive performance at follow-up in women (mean age: 65.8 ± 9.3 years). These findings globally suggested potential sex differences in the relationship between sleep duration and the risk of cognitive decline.
Further supporting the detrimental effects of extreme sleep durations on cognitive performance, Wu et al. (2021) [21] analyzed data from 16,948 Chinese men and women, aged 45 to 74 y.o. at baseline from the Singapore Chinese Health Study cohort. Sleep duration was evaluated at three time points: baseline (1993–1998), follow-up 2 (2006–2010), and follow-up 3 (2014–2016). At follow-up 2, individuals identified as presenting a long sleep duration (≥ 9 h per night) at baseline were associated with a higher risk of cognitive impairment (OR = 1.43; 95% CI: 1.24–1.66), compared to individuals who presented 7 h of sleep per night. At follow-up 3, individuals presenting both long (≥ 9 h per night) and short (≤ 5 h per night) sleep (OR = 2.03 and 1.26, respectively) showed a significant increased risk of presenting cognitive impairment. This finding reinforced the previously documented U-shaped relationship between sleep duration and cognitive performance. Authors also analyzed changes in sleep patterns documented at the different time points of the study and the risks associated with the change from a sleep duration group to another during the longitudinal observation. Specifically, participants who extended their sleep duration from short (≤ 5 h/night) to long (≥ 9 h per night) from baseline to follow-up 2 presented a 2.18-fold higher risk of developing cognitive impairment. Similarly, those who transitioned from a recommended sleep duration (7 h/night) to a long sleep duration had a 1.55-fold increased risk. The greatest risk, notably, was observed among individuals who reduced their sleep from long (≥ 9 h/night) to short (≤ 5 h/night), with 2.93-fold higher odds of developing cognitive impairment.
The study by van Oostrom and colleagues (2018) [22] evaluated the sleep habits of middle-aged adults (mean age 55.2 ± 6.9 years) and documented that a long sleep duration (≥ 9 h) was significantly associated at the follow-up with poorer global cognitive function (β = −0.06; CI: −0.11 to − 0.02), memory abilities (β = −0.09; CI: −0.16 to − 0.01), and cognitive flexibility (β = −0.07; CI: −0.14 to − 0.01). Additionally, both short (≤ 5 h/night) and long (≥ 9 h) sleep durations were associated with lower cognitive processing speed among individuals who frequently reported not feeling rested at awakening. Moreover, long sleepers (≥ 9 h per night) scored lower in cognitive flexibility compared to those with an intermediate/normal sleep duration (7–8 h) [22]. In multivariable linear regression models, changes in self-reported sleep duration were evaluated in association with the cognitive function at follow-up. Although long sleep duration was initially associated with reduced cognitive function at the longitudinal observation, no significant associations were found between changes of sleep duration and changes in cognitive function over time [22]. These findings suggest that, in middle-aged adults, the relationship between sleep duration and cognition may be more complex and distinct from the patterns typically observed in older adults.
Xu et al. (2014) [23] involved in their study 13,888 participants (mean age ± SD: 63.2 ± 6.4 years for men and 59.9 ± 6.6 years for women), with an average follow-up of 4.1 years. Authors investigated the association between both short sleep duration (≤ 5 h/night) and long sleep duration (≥ 10 h/night) with the memory performance, as measured by the Delayed 10-Word Recall Test (DWRT), and the cognitive status, as evaluated by the Mini-Mental State Examination (MMSE), measured at follow-up. The study found that only short sleep duration (≤ 5 h/night) was significantly associated at follow-up with an increased risk of developing memory deficits, defined as a DWRT score < 4. The OR for developing a memory deficit was 1.53 (95% CI: 1.21–1.93) for short sleepers compared to those with normal sleep duration (7 h/night). Compared to a frequency of daytime napping of 1–3 times per week, individuals who presented a daily nap showed a higher risk of memory impairment at follow-up– measured by DWRT (adjusted OR = 1.34 [1.06–1.69]).
Beyond sleep duration and in agreement with the latter results documented by Xu et al. [23], Nakakubo et al. (2019) [24], in their 4-year longitudinal study of 3,151 older adults aged 65 or older, explored the impact of sleep duration and excessive daytime sleepiness (EDS) on cognition. EDS was identified by the Authors when the participants answered “almost always” to the question “How often do you experience daytime sleepiness requiring a nap?”. Conversely, answers “almost always”, “sometimes” and “rarely or never” were not considered as EDS. On the one hand, Authors showed that both short (≤ 6.0 h/night) and long (≥ 9.0 h/night) sleep durations were linked to a higher risk of cognitive decline at follow-up compared to intermediate/normal sleep time (6.1–8.9 h/night). Moreover, incidence of cognitive decline at follow-up significantly varied across the sleep duration groups (short sleep: 15.9% [n = 35], intermediate sleep: 11.9% [n = 191], long sleep: 20.1% [n = 54]; p = 0.001). On the other hand,participants with EDS (prevalence: 13.1%) had a significant decline of cognitive performance at follow-up compared to participants without EDS (18.9% vs. 12.5%, p = 0.004).
Similarly, Jaussent et al. (2012) [25] showed in a large sample of participants aged 65–85 y.o. that EDS increased the risk for cognitive decline (a 4-point reduction in MMSE scores during the 2-, 4-, and 8-year follow-up) at follow-up by 26% (OR = 1.26, 95% CI = 1.02–1.56). Moreover, in the analysis of baseline data of subjects who developed dementia during the follow-up, EDS contributed with an higher risk (39%). This association remained significant in the fully adjusted model, accounting for confounding factors, including the use of prescribed sleep medications. Unexpectedly, difficulty maintaining sleep was negatively associated with cognitive decline at follow-up [25], a finding the Authors suggested may be confounded by cholinesterase inhibitors treatment during the follow-up period. No significant associations were found between sleep disturbances (components of insomnia and daytime sleepiness) and declines in visual memory performance or verbal fluency over the 8-year follow-up period.
P. Sung et al. (2017) [26] conducted a retrospective study involving patients (mean age 48.6 ± 16.2 y.o.) with non-apnea sleep disorders (NSD), defined as insomnia, hypersomnia, circadian sleep-wake rhythm disorders, other non-organic sleep disorders. Authors found significant higher dementia risk in patients with NSDs compared to subjects without sleep disorders (adjusted HR 1.46; 95% CI: 1.38–1.54; p < 0.0001). The risk for dementia was highest within the first year following a NSD diagnosis but remained higher even after 5 years of follow-up compared to those without a NSD diagnosis (adjusted HR 1.44; 95% CI: 1.32–1.57; p < 0.0001).
SDB was also examined in the “Prevention of Alzheimer’s Disease with Vitamin E and Selenium” (PREADViSE) study by Ding et al. [27], which investigated the association between self-reported sleep apnea and the risk for dementia in the male population included and aged 62 years and older. Participants initially underwent a cognitive screening with the Memory Impairment Screen (MIS), and those who were positive to memory impairment proceeded to second-level screening (CERAD-e or TICS-m). The study found that, among participants without the apolipoprotein E (ApoE) ɛ4 allele, baseline self-reported SDB was associated with a 66% higher risk of developing dementia at follow-up. In contrast, no additional risk was observed in participants carrying the ApoE ɛ4 allele. Further analysis adjusting for confounding factors showed that self-reported SDB remained significantly associated with an increased risk of presenting dementia at follow-up. Although the cumulative incidence was higher in the SDB group (24.4%) compared to the group without SDB (9.3%), the difference was not statistically significant, possibly due to the limited number of dementia cases documented at follow-up (p = 0.14 by log-rank test). In the adjusted model, the history of SDB presented a trend toward significance (HR = 1.44; 95% CI: 0.96–2.17; p = 0.08). Specifically, men with SDB tended to show a higher likelihood of developing dementia compared to men without SDB, suggesting that sleep apnea may increase dementia risk, particularly in individuals without the ApoE ɛ4 allele.
Focusing on insomnia, Beydoun et al. (2021) [28] analyzed the Health and Retirement Study (HRS) data and found that severe insomnia symptoms at baseline in participants aged ≥ 65 years were associated with an increased risk of physician-diagnosed memory problems (HR = 1.21, 95% CI: 1.02–1.44) at the follow-up, performed over a 10-year period. Specifically, individuals who experienced an increase in the severity of insomnia symptoms over time had a 41–72% higher risk of presenting physician-diagnosed memory problems and a 45–58% higher risk of dementia diagnosis based on HRS criteria.
Finally, Lee et al. (2022) [29] conducted a longitudinal retrospective cohort study using the uniform dataset collected by the National Alzheimer’s Coordinating Center. The results showed that older adults with sleep disturbances had a higher likelihood of developing dementia during an average follow-up of 4.5 years, particularly among those with normal cognition at baseline (HR 1.56, 95% CI: 1.07–2.27). Furthermore, greater severity of sleep disturbances was correlated with an increased dementia risk (HR 1.40, 95% CI: 1.05–1.86).
Actigraphic studies
The main characteristics of the selected studies with objective sleep measurements are summarized in Table 3. Lysen and colleagues [30] investigated the association between actigraphy-estimated sleep parameters and 24-hour activity rhythms and the risk of dementia in a cohort prospectively evaluated (mean age 66 ± 8 y.o., 53% women). Their findings showed that longer sleep latency (HR per one standard deviation increase: 1.44, 95%, CI: 1.13–1.83) and more time spent in bed (HR: 1.40, 95% CI: 1.04–1.88) documented at the baseline investigation were associated with a higher risk of developing dementia over a 11.2 year of follow-up. In contrast, higher sleep efficiency (HR 0.72, 95% CI 0.55–0.93) and later “lights-off” times (HR 0.56, 95% CI 0.41–0.76) were associated with a lower risk of developing cognitive decline. Moreover, a later timing of onset of the least active 5 consecutive hours (L5), a non-parametric circadian rhythm analysis parameter, was associated with a reduced risk of dementia during the first 2 years of follow-up (HR: 0.23, 95% CI: 0.09–0.61). Notably, total sleep duration itself was not significantly associated with higher dementia risk (HR: 0.97, 95% CI: 0.74–1.29) or AD risk (HR: 0.92, 95% CI: 0.68–1.26). No associations were observed between circadian sleep-wake rhythm and the higher risk of dementia, even after adjusting for potential confounders such as SDB, number of daytime naps, or ApoE ε4 allele.
Table 3 Main characteristics of the selected studies using objective sleep measurementsThe study by Chen et al. (2022) [31] analyzed 7-day accelerometry data from 72,242 participants in the UK Biobank (54.9% women; mean age 62.1 y.o.). The authors calculated the relative circadian amplitude, which is a measure of circadian sleep-wake rhythm disruption, and found that individuals with reduced relative amplitude exhibited an increased risk of developing dementia after a median follow-up of approximately 6.1 years (HR 1.22 [95% CI 1.14–1.29], p < 0.001).
Finally, Peng Li et al. (2023) [32] documented that older adults tended to take longer and more frequent daytime naps. Using actigraphy, they found that the progression of AD accelerated the age-related increase in nap duration and frequency. Moreover, longer daytime naps were significantly associated with an increased risk of developing AD, with a HR of 1.20 (95% CI: 1.06–1.35; p = 0.004) for each one standard deviation increase in nap duration. Similarly, a higher daytime nap frequency was also linked to a greater AD risk (HR:1.23; 95% CI: 1.08–1.39; p = 0.001) for each one standard deviation increase in nap frequency. Interestingly, their study identified a bidirectional relationship between excessive daytime napping and cognitive decline. More excessive napping was correlated with worse cognition one year later, while worse cognition was in turn associated with increasing napping in the following year [32].

Comments (0)