In this systematic review of pediatric laparoscopic cholecystectomy (LC), we found that gallbladder perforation with stone spillage occurs in approximately 4.3% of procedures, and clinically significant retained-stone complications arise in about 1.7% of children. These findings underscore that, although uncommon, dropped or retained gallstones in the pediatric population carry nontrivial risks of abscess formation, biloma, and choledocholithiasis—complications that may present weeks to years after the initial surgery.
Our spillage rate aligns closely with large adult series, in which stone loss during LC has been reported in 5–6% of cases [20]. Likewise, the retained-stone complication rate in adults ranges from 0.08 to 2.3% [21], suggesting that children are not spared these risks. Yet, pediatric patients may manifest sequelae differently; for example, the cases we reviewed included very late presentations up to two years post-LC [19], a feature less commonly documented in adult cohorts.
Several factors likely contribute to pediatric stone spillage and retention. Hemolytic disorders such as sickle-cell anemia disrupt bile composition and gallbladder motility, predisposing to fragile gallbladders and small, pigment-rich stones that may fragment intra-operatively [7]. Indeed, our subgroup analysis hinted at a modestly higher spillage rate in sickle-cell cohorts (6.4%) versus non-hemolytic populations (4.0%). Moreover, technical variables—including the use of retrieval bags, irrigation protocols, and surgeon experience—evolved over the study period. Later series utilizing the “Critical View of Safety” and fluorescence cholangiography reported numerically lower rates of spillage and retained stones, although direct causal inference is limited by observational design.
The clinical implications are clear: meticulous intra-operative technique and vigilant postoperative surveillance are warranted. When stone spillage is recognized, surgeons should attempt complete retrieval with suction, irrigation, and retrieval bags; detailed operative notes flagging any spill can prompt early imaging if patients develop unexplained pain or sepsis. Ultrasound sufficed for superficial abscesses, whereas CT and MRCP were invaluable for deeper collections or ductal stones, guiding definitive management such as percutaneous drainage or ERCP clearance. All reported pediatric cases in our review achieved full recovery following targeted intervention.
Using the GRADE framework, we judged the certainty of both primary outcomes—stone-spillage incidence and retained-stone complications—to be low because of three factors: (1) study limitations and moderate-to-high risk of bias, (2) imprecision stemming from small event counts and wide confidence intervals, and (3) inconsistency reflected in residual heterogeneity even after random-effects, subgroup, and leave-one-out analyses. Consequently, the pooled percentages should be regarded as approximate guidance rather than definitive rates.
Several issues likely underlie the heterogeneity. Key confounders—hemolytic disorders, obesity, surgeon experience, evolving instrumentation, and variable follow-up—were seldom measured or adjusted for. Most cohorts were small (< 150 patients, only three ≥ 200), which further reduces statistical power, widens confidence intervals, and limits multivariable adjustment.
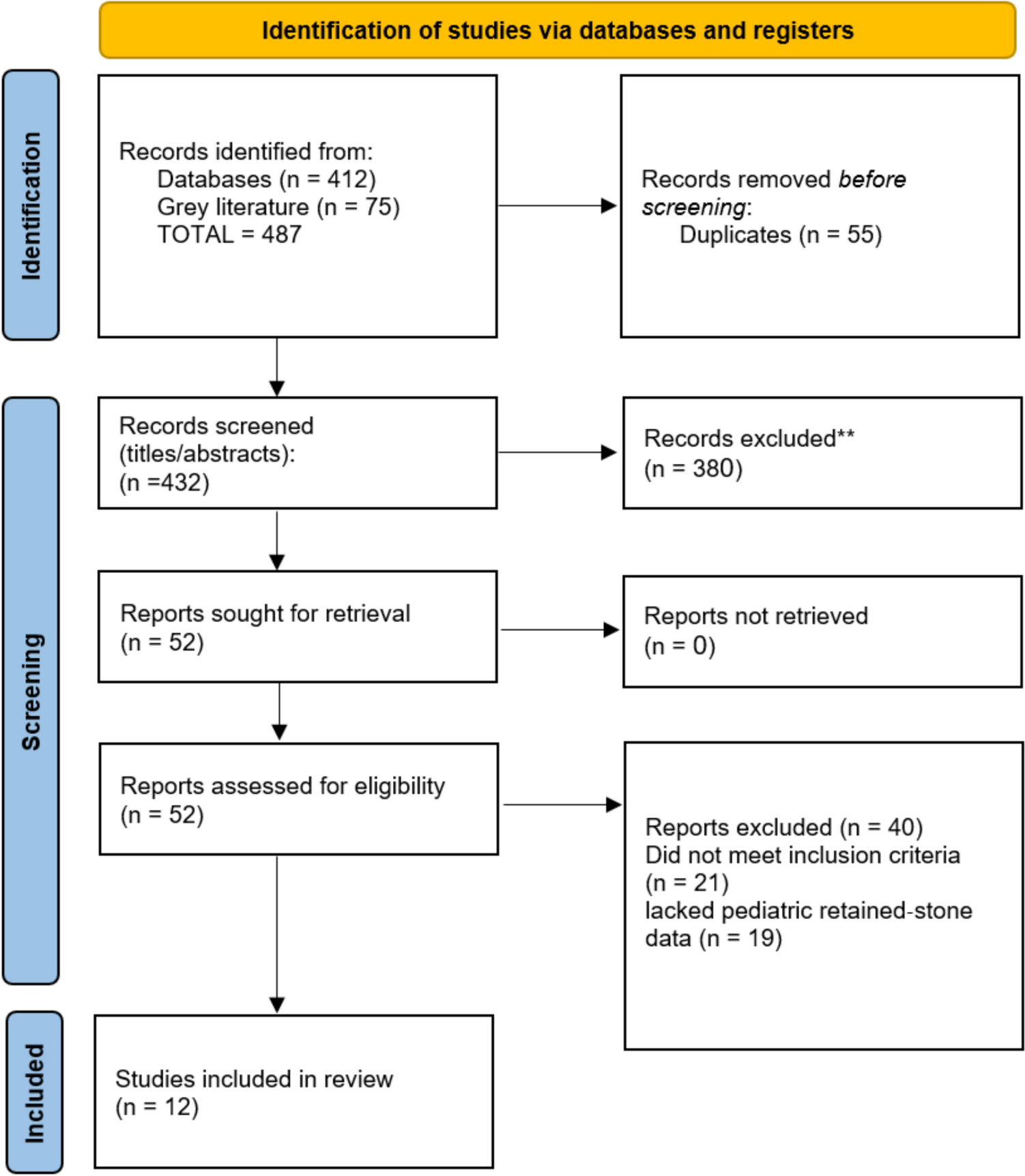
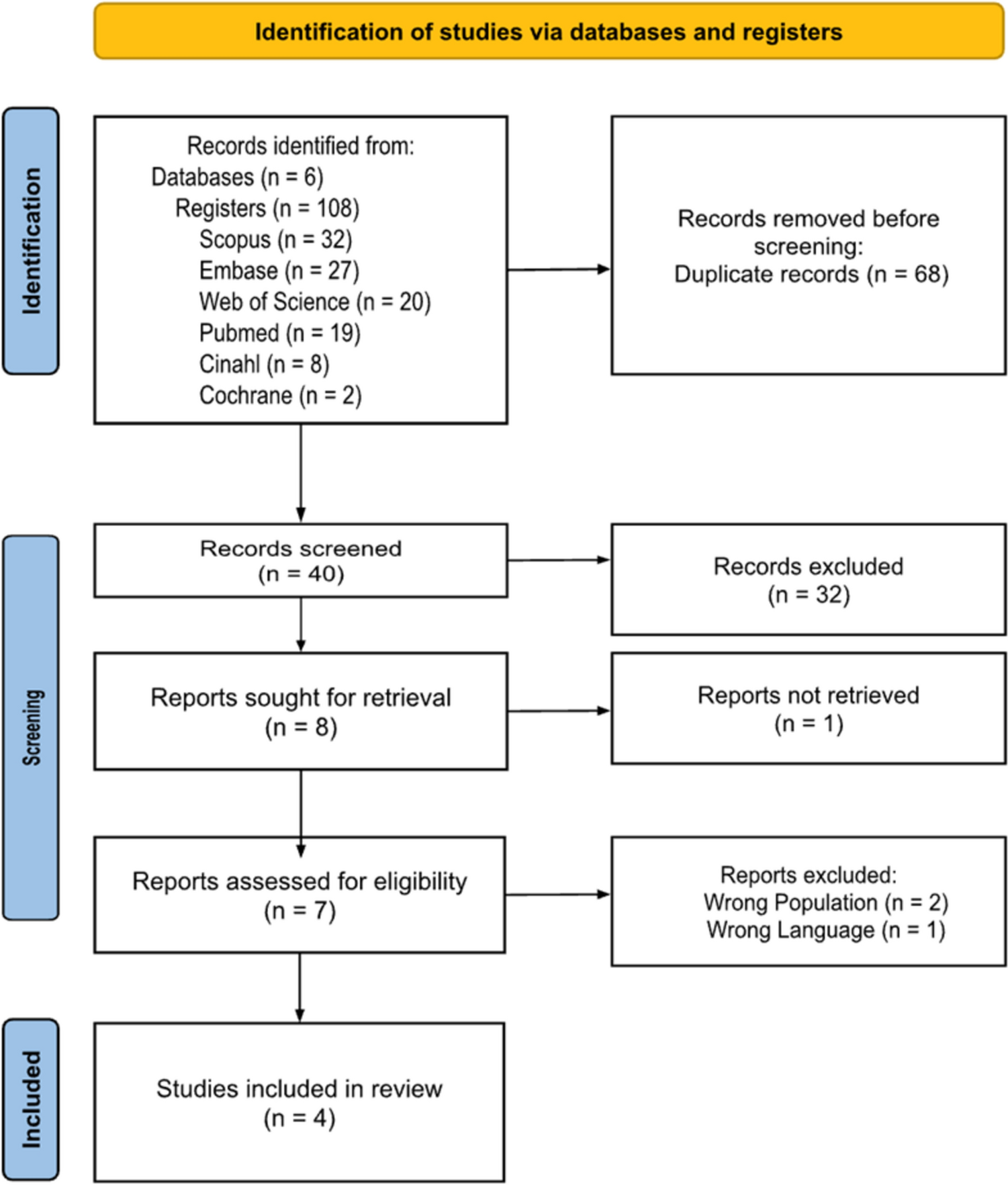
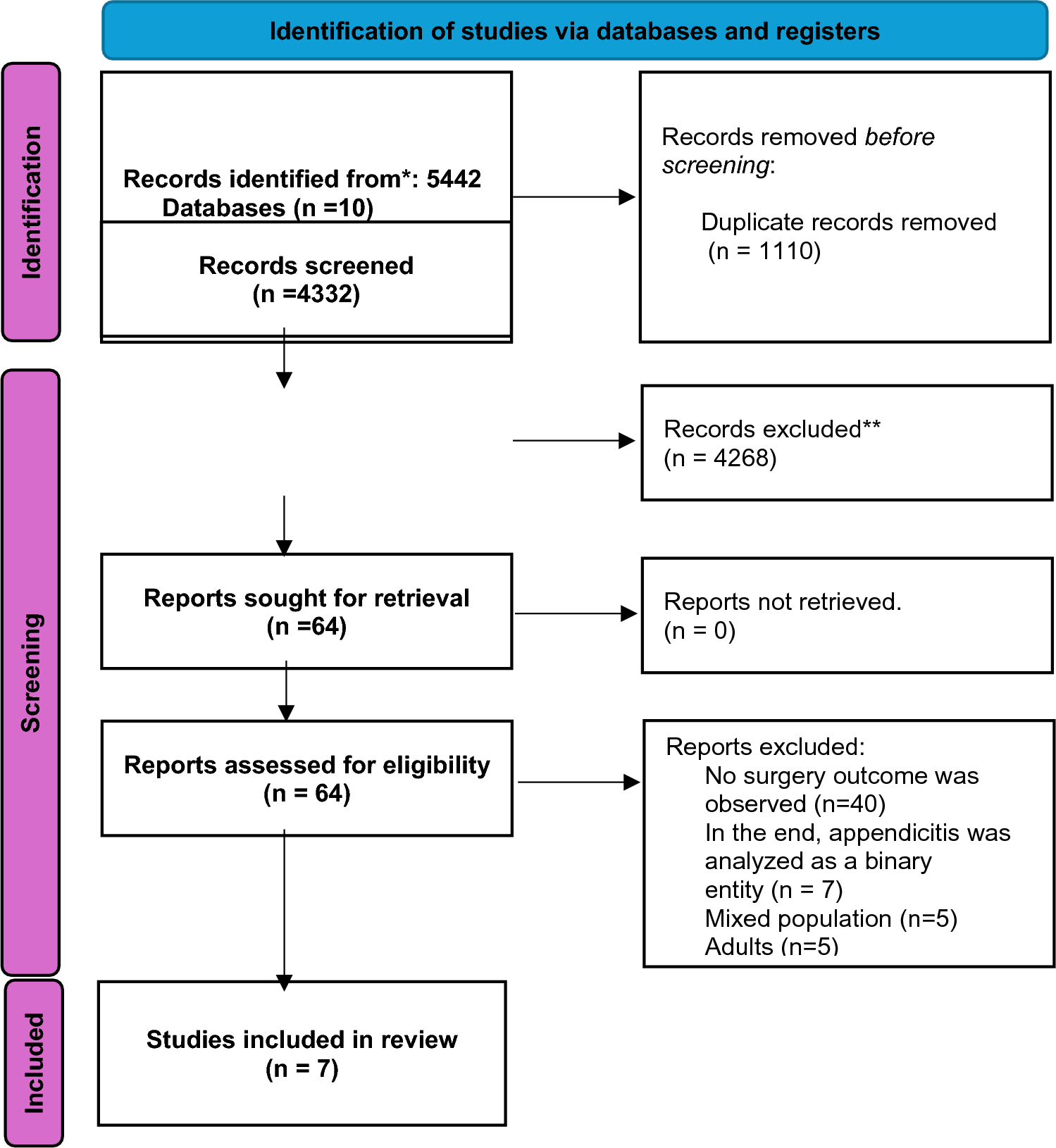
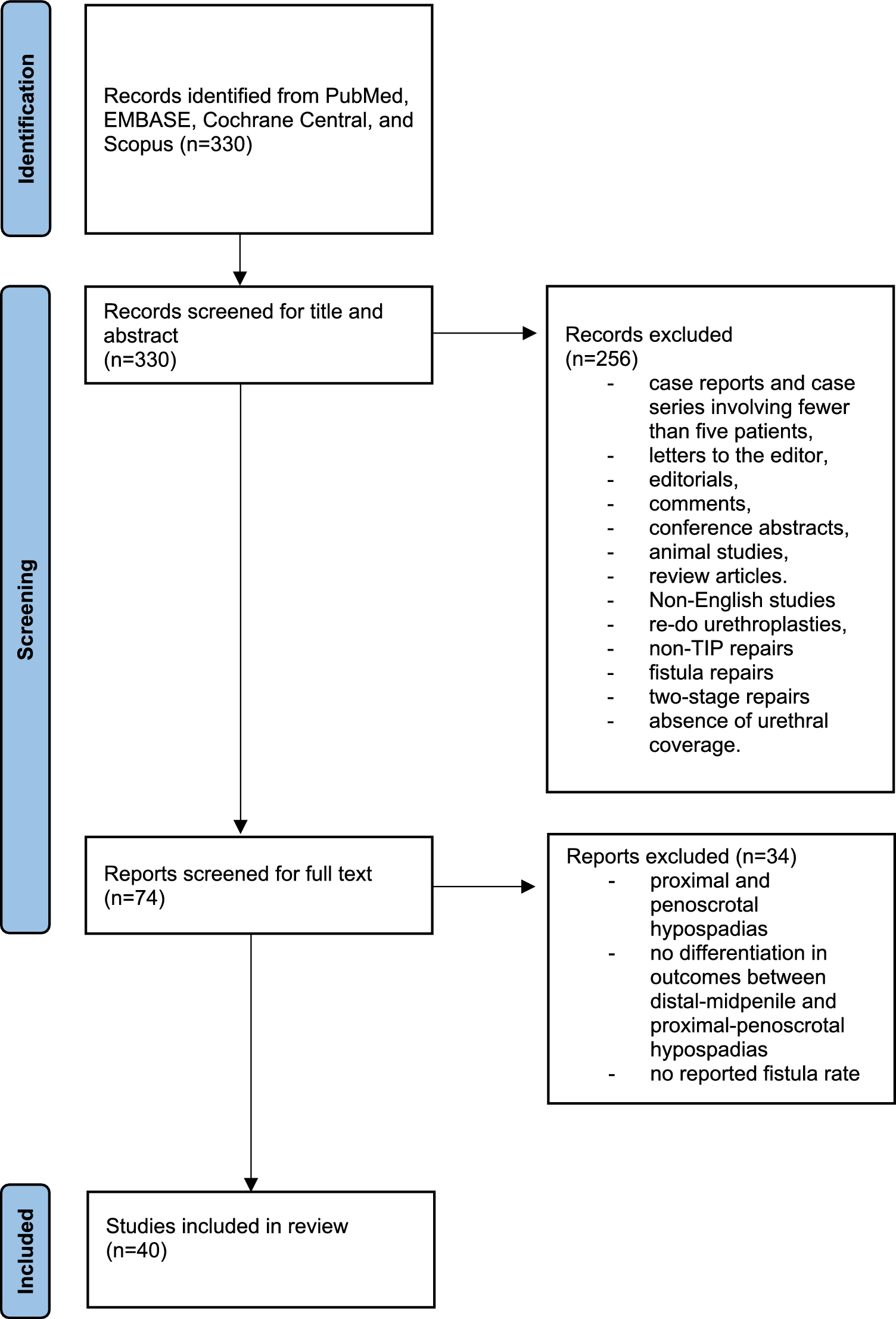
Despite these limitations, the review has notable strengths: strict adherence to PRISMA reporting standards, a comprehensive multi-database and gray-literature search, and systematic risk-of-bias appraisal with ROBINS-I and JBI tools [22]. Nonetheless, all included studies were observational (predominantly retrospective) with inconsistent follow-up beyond discharge; heterogeneous outcome definitions and technical details restrict precision; and publication bias could not be assessed reliably [23]. Given these constraints, all clinical recommendations should be interpreted as conditional pending high-quality, prospective multicentre data.
Future research should focus on prospective multicenter registries with standardized definitions of stone spillage and retention, uniform follow-up protocols, and core outcome sets encompassing abscess formation, biloma, ductal stones, and reintervention rates. Such efforts would enable robust risk-factor analysis and potentially set the stage for randomized trials of retrieval adjuncts (e.g., irrigation versus endobag use).
This review demonstrates that retained gallstones after pediatric LC, though infrequent, pose significant clinical challenges. Surgeons should maintain a high index of suspicion for spilled stones, document any intra-operative leakage meticulously, and employ appropriate imaging and intervention strategies to mitigate morbidity in this vulnerable population.

Comments (0)