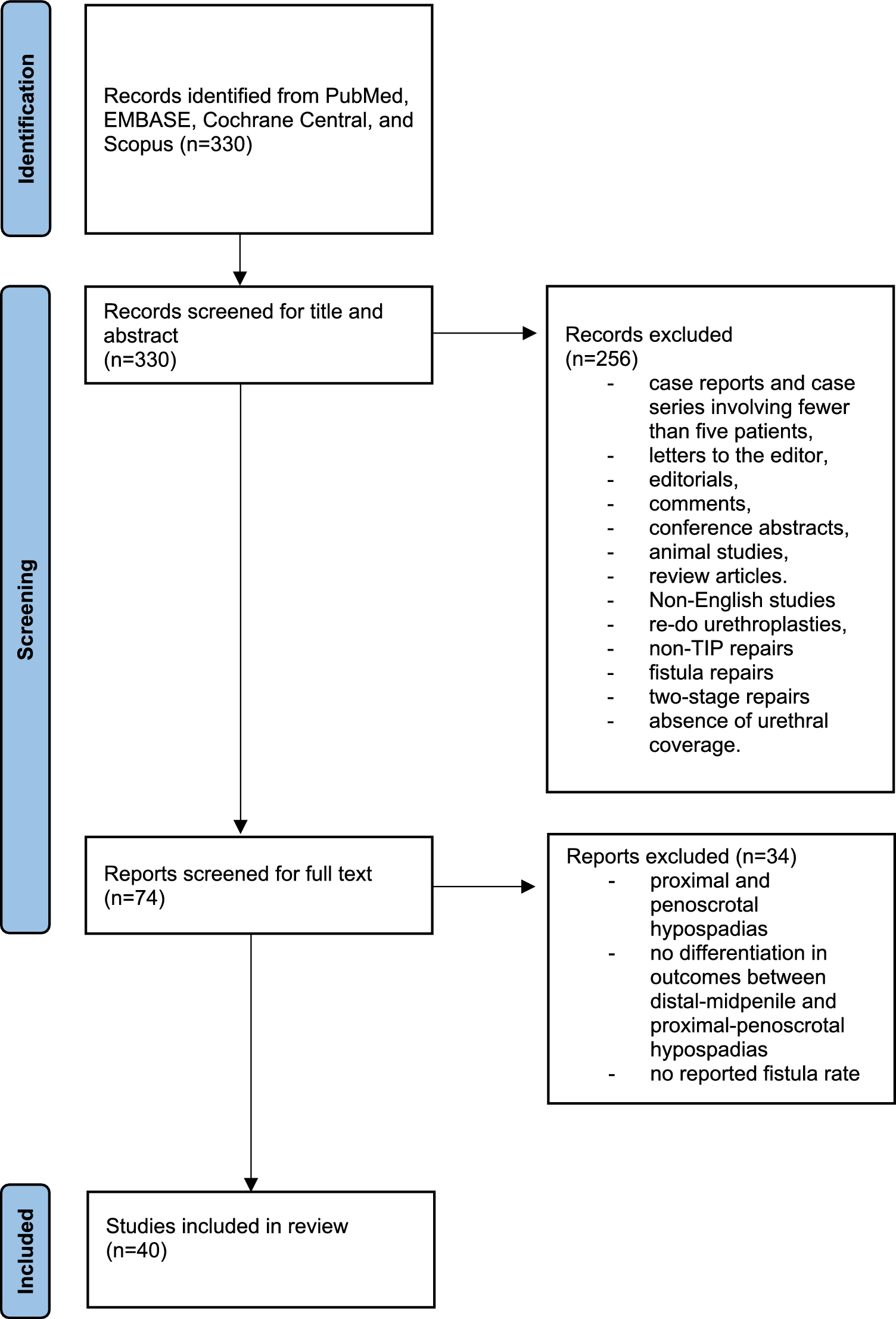
Characteristics of included studies
A total of 40 studies were identified, which addressed the postoperative complications of primary repair of distal and midpenile hypospadias after TIPU repair, with a single or double layer for neo-urethral coverage. These studies included 5920 patients. Half of these studies were published within the past decade, and all of them were published between 2002 and 2024. The study design was retrospective for 18 articles, prospective for 14, and RCTs for 8.
Patients’ median follow-up durations varied from 4.5 to 57.6 months, while their mean ages ranged from 0.9 to 12.2 years.
Fourteen articles addressed exclusively distal hypospadias, ten articles addressed both distal and midpenile hypospadias with a distinction in outcomes, and sixteen articles addressed both distal and midpenile hypospadias without a distinction in outcomes.
In eleven articles, all patients received the same type of single or double layer. In the remaining articles, patients received either the same type of layer in single or double format, single layers of a different type, double layers of a different type, or a combination of single and double layers using different tissues.
For this reason, we grouped together all patients in the same study who received the same type of layer for neo-urethral coverage and conducted the analysis by comparing these homogeneous groups.
Details of included articles are available in Table 1.
Table 1 Included articlesComplication rates in distal hypospadias repairSingle layer
Nineteen studies examined single-layer neo-urethral coverage, with seven of them implementing various tissues across different patient groups [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23]. Consequently, 27 homogeneous groups were identified. Postoperative UCF rates varied widely, from 0% to 38.5%. Five groups recorded no fistulas, six groups showed rates below 5%, ten groups ranged from 5% to 10%, and six groups exceeded a 10% rate. Data on meatal stenosis were missing for five groups; among those with data, stenosis rates ranged from 0% to 33.3%, with 0% in seven groups, 0–5% in nine, 5–10% in four, and over 10% in two. Wound dehiscence was uncommon, observed in six groups with rates from 1.2% to 6.3%. Skin necrosis was rare, appearing in only two groups at rates of 2.4% and 3.6%.
Dorsal dartos (DD) flap
The primary single-layer applied was the dorsal dartos (DD) flap, used across 15 groups [5,6,7, 9,10,11,12,13,14, 16,17,18,19,20,21]. Among these, two groups observed no postoperative UCFs, three reported rates below 5%, and seven noted rates between 5% and 10%. Higher fistula rates were documented in the remaining groups, particularly in studies by Verma et al. [5] (20.0%), Yildiz et al. [6] (23.1%), and Naumeri et al. [18] (23.8%). Conversely, the incidence of meatal stenosis was minimal, with the highest noted in the article by Hamid et al. [13] (10.0%).
Alternative layers
Alternative layers were less frequently adopted. The ventral dartos (VD) flap was used in four groups [14, 15, 17, 19], showing a fistula rate from 2.3% to 14.3% and stenosis rates described in two groups at 0% and 2.3%. TV was applied in one group [19] without any postoperative fistulas or stenosis, while Buck’s fascia, also used in a single group [13], had fistula and stenosis rates of 2.4% and 3.6%, respectively. The glanular subcutaneous tissue was described in one group [15] with a fistula rate of 38.5%. Finally, spongioplasty was evaluated in four groups [5, 20, 22, 23]; three reported low fistula rates (0–2.5%) and stenosis rates ranging from 0% to 12.5%, while one group noted a fistula rate of 26.7% and a stenosis rate of 33.3%.
Double layer
In 13 studies, the double-layer technique was utilized, and the same tissues were used across patients in the individual studies [6,7,8,9,10,11, 16, 18, 24,25,26,27,28]. UCF rates ranged from 0% to 12%. Of the patient groups, seven had no fistulas, four had rates between 0% and 5%, one had a rate of 5–10%, and one exceeded 10%. Meatal stenosis rates ranged from 0% to 11.1%, with seven groups showing no cases, four groups between 0% and 5%, one group between 5% and 10%, and one group with more than 10%. Wound dehiscence, observed in four groups, had rates from 2.1% to 3.5%, while skin necrosis did not occur in any group.
Double dorsal dartos (DD) flap
The double DD flap was the most used, applied in 8 groups [6,7,8,9,10, 18, 24, 27]. In this cohort, seven groups reported no postoperative fistulas, while only one group observed a fistula rate of 3.7%. In contrast, meatal stenosis rates were slightly elevated in three groups, ranging from 2.1% to 11.1%, while the remaining groups reported no stenosis.
Alternative layers
Other double-layer techniques were used less frequently. The combination of DD flap with spongioplasty or periurethral tissue was used in two groups [16, 26], showing variable rates of complications: fistula rates ranged from 3.3% to 8.3%, and stenosis rates from 0% to 8.3%. The de-epithelialized dorsal prepuce, also used in two groups [25, 28], presented low complication rates, with fistula rates of 2.1% and stenosis rates from 1% to 2.1%. Finally, foreskin reconstruction was used in one group [11], resulting in a fistula rate of 12% and no cases of stenosis.
Complication rates in midpenile hypospadias repairSingle layer
Among seven studies investigating single-layer techniques for midpenile hypospadias, three applied distinct single layers across various patient groups [15, 18,19,20,21,22,23]. Consequently, ten homogeneous groups were identified. Across the groups, UCF rates ranged from 0% to 36.4%. Three groups had no fistulas, one group had rates between 0% and 5%, one group showed rates of 5–10%, and five groups exceeded 10%, with rates between 12.5% and 36.4%. In terms of meatal stenosis, three groups did not report on it, while none of the remaining groups experienced any cases. Wound dehiscence was uncommon but reported in one group, with an incidence of 9.1%. None of the groups showed cases of skin necrosis.
Several tissue types were applied for neo-urethral coverage. The DD flap was used in three studies [18, 19, 21], showing high UCF rates between 12.5% and 36.4%, with no cases of meatal stenosis reported. The VD flap, used in one study [15], showed a fistula rate of 6.3%. TV, utilized in two studies [19, 20], resulted in low fistula rates (0–3.1%) and no occurrences of stenosis. Glanular subcutaneous tissue was described in one study [15], where 23.1% of patients developed postoperative fistulas. Finally, spongioplasty alone was applied in three studies [20, 22, 23], with two reporting no fistulas or stenosis and one reporting a 16.7% fistula rate with no stenosis.
Double layer
Four studies examined double-layer techniques, with one study applying different layers in two patient groups [18, 26,27,28]. Therefore, five groups were reviewed, and UCF rates ranged from 0% to 30.8%. Two groups showed no fistulas; two groups had rates between 0% and 5%, while one group reported a rate of 30.8%. Meatal stenosis data were unavailable for two groups; the other groups reported no stenosis or rates below 5%. Wound dehiscence rates included two groups with no cases, two groups with rates below 5%, and one group at 6.3%. Skin necrosis was absent in four groups but observed in one, with an occurrence rate of 23.1%.
Various techniques were reported. The double DD flap, applied in two groups [18, 27], resulted in no cases of postoperative UCF or meatal stenosis. In the single group, where the DD flap combined with spongioplasty or periurethral tissue was used [26], the reported complication rates were 30.8% for fistulas, 23.1% for skin necrosis, and 3.8% for both stenosis and wound dehiscence. The combination of TV with spongioplasty or periurethral tissue, utilized in one group [26], resulted in lower rates of 4.8% for fistulas, stenosis, and wound dehiscence. Finally, de-epithelialized dorsal prepuce, used in one group [28], showed rates of 4.2% for fistulas, 3.2% for stenosis, and 6.3% for wound dehiscence.
Complication rates in studies with combined outcomes for distal and midpenile hypospadiasSingle layer
Thirteen studies reported on single-layer neo-urethral coverage, with three using distinct layers across different patient groups [29,30,31,32,33,34,35,36,37,38,39,40,41]. As a result, we identified 16 groups, in which UCF rates varied from 0% to 24.3%. A single group had no fistulas, two groups had rates between 0% and 5%, seven groups ranged from 5% to 10%, and six groups exceeded a 10% rate. Meatal stenosis rates spanned 0–11.1%, with 0% in three groups, 0–5% in seven, 5–10% in four, and above 10% in two. Wound dehiscence occurred in six groups at rates from 0% to 5%, while two groups experienced higher rates of 5.6% and 10.8%. Skin necrosis was noted only once, with a 2.7% rate.
Dorsal and ventral dartos flap
The DD flap and VD flap were used in seven [29,

Comments (0)