This is one of the largest series addressing the surgical management of Müllerian duct remnants, to date. This is an area where literature is sparse, and neither comparisons between the two techniques nor selection criteria for them have been published [8], and most reports (especially about division) are singular cases [28]. In this study, we introduced a novel classification system, the G–VD–MDR, to guide the surgical management of MDRs in male patients with DSD. Setting the scene and context for this work, it is important to note that, intuitively, an excision is ideal for those cases, being raised as males, thus not needing this structure, and owing to the potential concerns around the MDR presence, i.e. including the potential for malignant degeneration [7, 29, 30], voiding problems [26], urinary tract infection and epididymitis/epididymo-orchitis [6, 27] (which was present in 6 of our cases) and anchoring undescended testes abdominally [9, 25, 30, 31] (which was unanimously present in all our cases); however, the trade-off of accepting a division may be dictated by the configuration [3, 12, 28, 32]. Our results indicate that bilateral MDR–vas deferens relations and higher EMS favour division, whereas cases with absent/unilateral MDR–vas deferens relations and lower EMS scores are more suited for near-total excision. The overall comparative outcomes between both groups are summarised in Table 6, illustrating the anatomical and functional rationale guiding each surgical approach. A survey of the available literature revealed that no unified anatomical scoring system currently exists to guide the surgical management of MDRs. Instead, reported approaches are often based on individual surgeon preference or intraoperative judgement, reflecting underlying anatomical principles but lacking standardisation. In this context, our proposed classification system seeks to consolidate these anatomical considerations into a structured and reproducible framework to support more consistent, evidence-based decision-making.
Comparison of both performed techniques in the current literature
In our study, 12 cases (67%) underwent MDR excision, aligning with the approach of Wei et al, done successfully in three cases [33]. Farikullah et al also recommended excision to achieve an orchidopexy while minimising the risk of malignancy [30] which they have done successfully in eight cases. On the other hand, some surgeons/authors, for the concern of damaging the vas deferens during its mobilisation from the MDR opt for leaving them in situ, as suggested by Vandersteen et al [17]; this argues the case for division or longitudinal splitting, consistent with the approach reported by El-Gohary, on 5 cases, where longitudinal splitting was successful to enable orchidopexy reaching the scrotum [34]. We have adopted this in 6 cases (33%). Raicevic et al [8] did an extensive systematic literature review to determine surgical outcomes, to find 10 articles over 10 years, reporting on 23 patients, where complete removal was done in 9 cases, near-complete removal in 11 cases and longitudinal splitting in 1 case, all reporting good outcomes. In recent years, robot-assisted techniques have also been employed for MDR excision in paediatric patients, offering improved dexterity and 3D visualisation, which may be particularly beneficial in cases with complex vas deferens relations [27, 35]. While not utilised in our cohort, robotic surgery may represent a valuable option in selected cases and has been increasingly adopted in other paediatric urological procedures [27, 35]. If a PU is involved, laparoscopic excision under cystoscopy guidance [20,21,22] could be considered.
Preoperative predictors of surgical decisionUtilising the EMS preoperatively
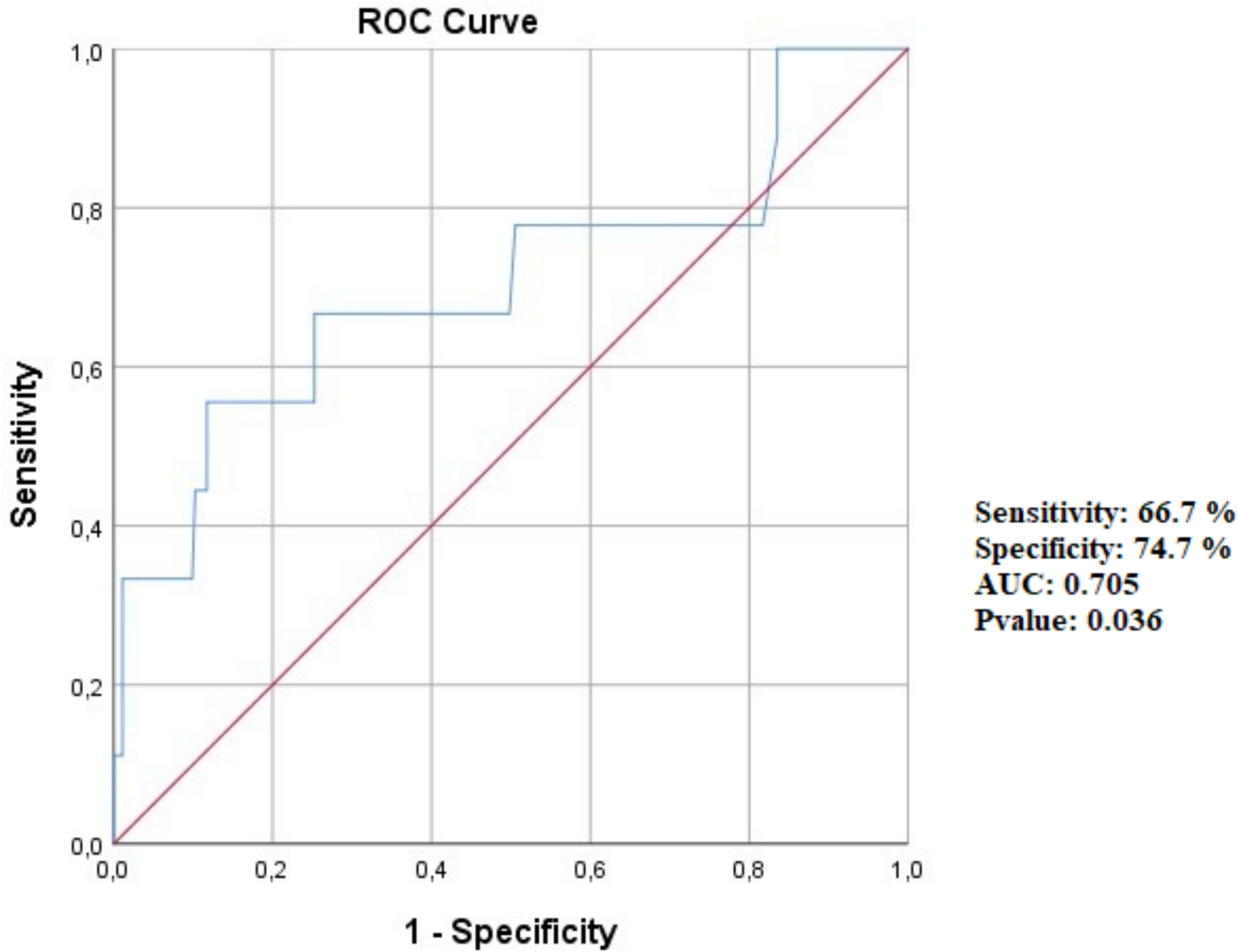
The mean EMS was significantly higher in cases that required MDR division (8.58 ± 1.74) compared to those that underwent excision (5.33 ± 1.98). Our findings suggest that a higher EMS correlates with (a) normal/adequate development of the male duct system (vas deferens), (b) a more complex MDR–vas deferens relationship, and c) a higher incidence of bilaterally normal gonads, making excision less safe. Therefore, a higher EMS favoured MDR division as the safer and more feasible option. In cases with 5.5 < EMS < 8.5, the decision cannot be reliably predicted before diagnostic laparoscopy. This observation can be attributed to testosterone production by Leydig cells, which is not only responsible for external genital virilisation but also plays a crucial role in mesonephric duct differentiation into the vas deferens [36].
Based on this correlation/relationship, we propose a surgical decision-making algorithm using EMS as a preoperative predictive tool. If the EMS is greater than or equal to 8.5, the case is usually suitable for division. If the EMS falls between 5.5 and 8.5, the surgical approach cannot be reliably determined preoperatively and awaits the diagnostic laparoscopy. If the EMS is less than or equal to 5.5, the case is usually suitable for excision if the patient is raised as a male. This would facilitate the surgeon’s preparedness preoperatively. This novel utilisation of the EMS system when retrospectively applied to the cases reported by Brandli et al [37], accurately predicted their surgical decisions. In their study, MDR division was performed in two cases of PMDS with an EMS of 10 to prevent injury or devascularisation of the male duct system, despite using a Pfannenstiel incision that could have facilitated excision, as their preference for division was guided by concerns for vas deferens preservation. Still one of their two cases needed a testicular microvascular auto-transplantation [37]. Contrarily, Wei et al [33] reported three cases of PMDS with EMS scores exceeding 10, yet still opted for excision, but had to adopt an open surgical approach, rather than laparoscopy, to achieve this.
Impact of karyotyping
Karyotypic subtypes associated with excision included 46, XY ovotesticular DSD, 46, XY MGD, 46, XY/45, XO MGD, and non-CAH 46, XY under-virilised males. In these groups, excision was feasible either due to absent or unilateral MDR–vas deferens relations with clearly defined courses that allowed safe dissection. These findings align with Krstić et al [38], who performed MDR excision in 3-out-of-4 cases of ovotesticular DSD assigned to the male sex, and with Tambo et al [39], who excised MDRs in 2-out-of-3 cases with 46, XY/46, XO mosaicism. Cases requiring division included 46, XY PMDS, where two patients had bilateral complex MDR–vas deferens relations, and a third had high-entry vas deferens on the left side. This finding aligns with Brandli et al [37] but contradicts Wei et al [33]. Division was also required in two non-CAH 46, XY under-virilised males with bilateral anatomically unclear vas deferens relations. In addition, in one case of 46, XX male, the MDR was elongated and closely applied to the vas deferens, precluding safe excision. See Supplemental Material—Table ST4 for further clarification, expanded and aggregate details.
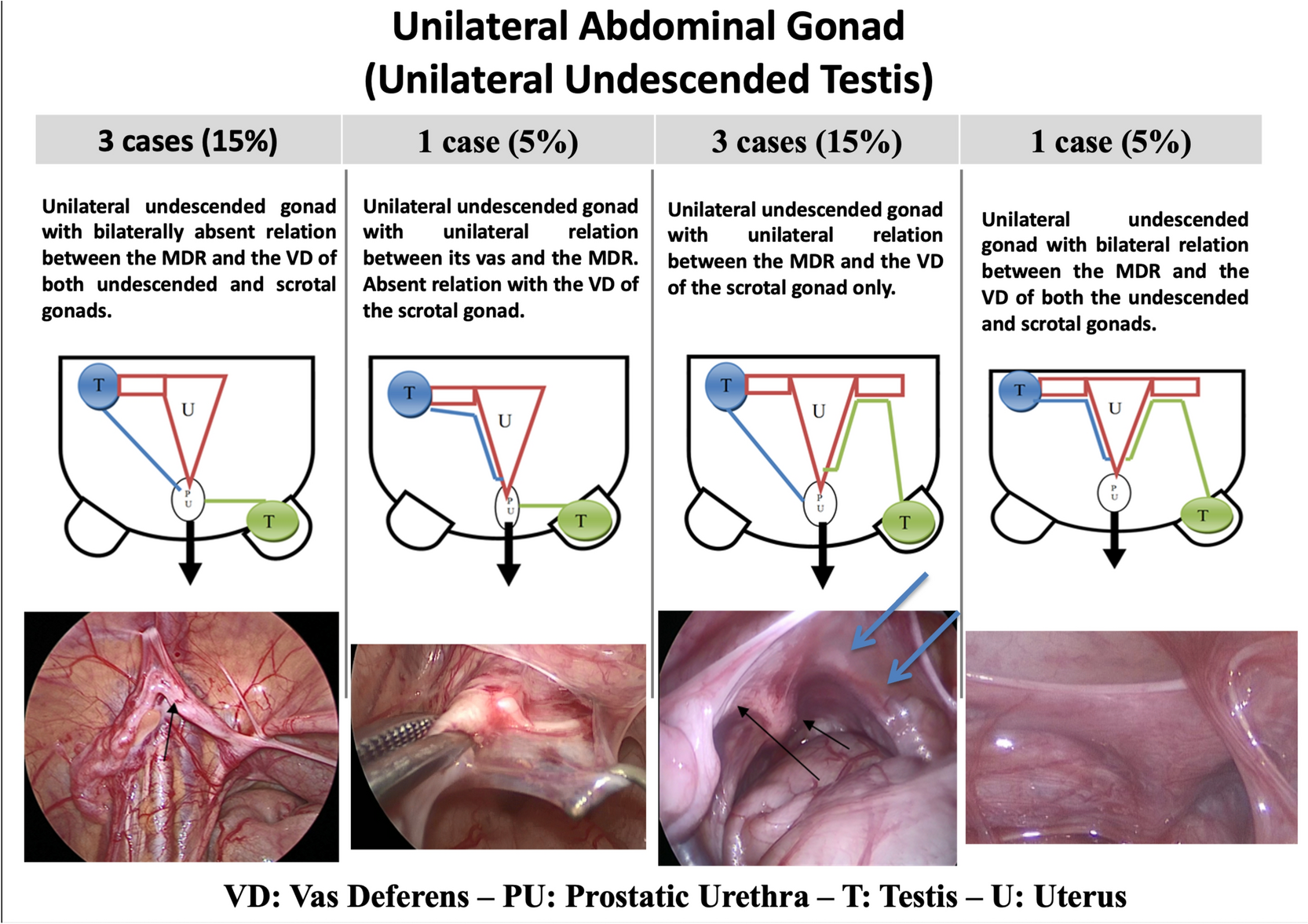
Intra-operative determinants of surgical decision
Our findings underscore that the intraoperative choice between excision and division is determined by MDR morphology, its relationship with the vas deferens, gonadal histopathology (whenever available), and prior knowledge of karyotyping and the EMS. To standardise surgical decision-making, we introduce the G–VD–MDR classification system, a novel anatomical classification framework based on diagnostic laparoscopy and gonadal biopsy. This system categorises MDR cases using three key parameters: Müllerian development (M1–M5), ranging from rudimentary remnants to a uterus with bilateral Fallopian tubes; vas deferens relation (V0–V2), reflecting the presence and complexity of MDR–vas deferens relations; and gonadal status (G0–G3), indicating absent, normal, dysgenetic, or ovotesticular gonads. For example, a case of PMDS with a uterus and bilateral Fallopian tubes (M2), a bilateral MDR–vas deferens relation (V2), and bilaterally normal testicular tissue (G1) can be classified as M2\V2\GR1\GL1. The proposed selection criteria for the surgical approach suggest that near-total excision is preferable when the vas deferens can be dissected from the lateral wall of the MDR, following it downwards and distally. The point of vas deferens entry should be well visualised, and excision should be performed above this point to preserve the vas deferens. Division or longitudinal splitting is performed using hook diathermy or preferably the harmonic scalpel or LigaSure™ (or equivalent) device. With the criteria generated from this work, in most future cases, the decision between excision and division can be made preoperatively or intraoperatively without staging, except where gonadal histology is essential to guide management.
Comparison of both performed techniques in our practice
A comparative analysis of excision and division highlights several advantages and disadvantages. Excision eliminates the risk of MDR-associated malignancy and reduces the incidence of recurrent urinary tract infections and epididymitis/epididymo-orchitis by removing lumen-bearing MDRs. However, it poses a higher risk of vas deferens injury due to increased manipulation and may fail still to achieve a complete removal, which can anchor gonads and hinder tension-free orchidopexy. Division, on the other hand, minimises vas deferens manipulation, reducing injury risk, and should decrease the risk of urinary tract infections by occluding the MDR lumen through cauterisation. In addition, it facilitates single-stage, tension-free orchidopexy by improving lateral mesorchium mobility. Nevertheless, the division procedure does not eliminate the risk of malignancy as MDR tissue is retained, necessitating vigilant follow-up with ultrasound or MRI. Electrocauterisation-induced fibrosis of the lining and lumen may hypothetically reduce malignancy risk but does not eliminate it. A detailed comparison of these outcomes is summarised in Table 6.
Limitations of the study
Despite the promising findings, a key limitation of this study is the relatively small sample size, which may impact the generalisability of the findings, although this would be one of the largest paediatric series published in this discipline [8]. The study lacks long-term follow-up data to assess potential complications such as infertility, malignancy, and recurrence of MDR-related pathology. From an operative outcome perspective, this study reports only on the early phase of that, and an extended follow-up is still required in subsequent future work. This would include an extended follow-up for fertility potential, testicular position and occurrence of epididymitis/epididymo-orchitis. Longitudinal studies assessing post-surgical outcomes, including reproductive function and malignancy risk, are essential to establish the long-term safety and efficacy of excision versus division. In addition, the retrospective application of the G–VD–MDR and EMS-based classification to previously operated upon cases, despite being prospectively sought for and planned, invites caution with its upcoming applicability in broader clinical settings, without a prospective trial for further validation. Future research should focus on multicentred studies with larger cohorts to validate the proposed classification system and refine its predictive accuracy.

Comments (0)