
Remember me

Postmortem magnetic resonance imaging (PMMRI) following fetal and perinatal demise is increasingly used in clinical practice as a non-invasive adjunct or alternative to autopsy. Imaging protocols vary widely between centers and there is currently no consensus.
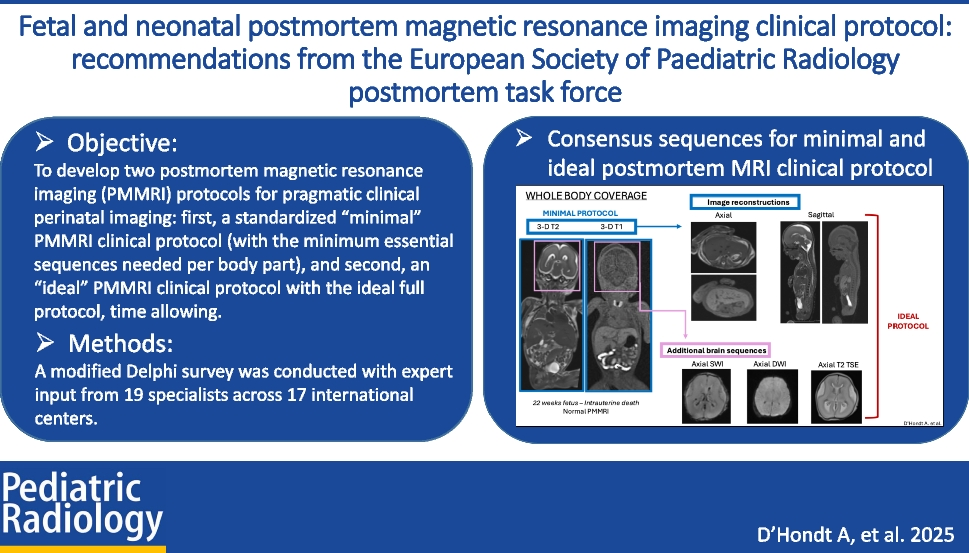
ObjectiveFrom expert consensus, we aimed to develop two PMMRI protocols for pragmatic clinical perinatal imaging: first, a standardized “minimal” PMMRI clinical protocol (with the minimum essential sequences needed per body part), and second, an “ideal” PMMRI clinical protocol with the ideal full protocol, time allowing.
Materials and methodsA modified Delphi survey was conducted, between July and November 2024, among members of the European Society of Paediatric Radiology (ESPR) postmortem (PM) Task Force, of the PM imaging committee of the Society for Pediatric Radiology (SPR) and the Australian and New Zealand Society for Paediatric Radiology (ANZSPR).
The survey was based on two pre-existing published PMMRI protocols and consisted of two multiple-choice tables which included all the MRI sequences in different planes according to each body part with an additional 10 PMMRI organizational questions (three of which were free text, seven multiple choice). An email containing the link to the survey was sent to 22 members of the different international PM imaging taskforces, recruited on a voluntary basis, given their clinical interest and experience in practicing perinatal PM imaging. The results were collected and analyzed in a descriptive manner, and a point-of-care PMMRI clinical protocol was established based on the recommendations of our expert panelists.
ResultsNineteen PM imaging specialists from 17 centers worldwide (Europe, the USA, Canada, Australia, and New Zealand) completed the survey and formed our expert panel. By consensus (defined as > 60% agreement), the final “minimal” PMMRI clinical protocol includes three-dimensional (3-D) isovolumetric T2- and T1-weighted sequences of brain (72.2% and 77.8% respectively) and chest-abdomen-pelvis (83.3% and 77.8% respectively). The “ideal” PMMRI clinical protocol includes 3-D isovolumetric T2- and T1-weighted sequences of the whole body (66.7—100%; 61.1 – 91.7% respectively) with axial susceptibility-weighted imaging (SWI) (81.3%) and diffusion-weighted imaging (DWI) (68.8%) of the brain. Additional sequence if time allows is axial T2 turbo spin echo (TSE) (56.3%) of the brain.
ConclusionAs a minimum, 3-D isovolumetric T1- and T2-weighted sequences of the brain and body, acquired together in a single station, should be performed as part of a perinatal clinical PMMRI protocol. We hope these recommendations will facilitate the standardization and globalization of perinatal PMMRI in clinical practice.
Graphical abstract
Comments (0)