
Remember me

A 28-year-old woman in her first pregnancy was referred to our fetal MRI unit after a third-trimester ultrasound revealed fetal brain hemorrhage.
Maternal history was positive for celiac disease under a gluten-free diet. Routine pregnancy follow‐up, including nuchal translucency, first‐trimester triple test, and first‐ and second‐trimester anatomy screening scans, was considered normal, with no evidence of hemorrhage or vascular malformation on Doppler sonography (last follow-up at 27 weeks gestational age). Amniocentesis was performed with a normal chromosomal microarray for a male fetus.
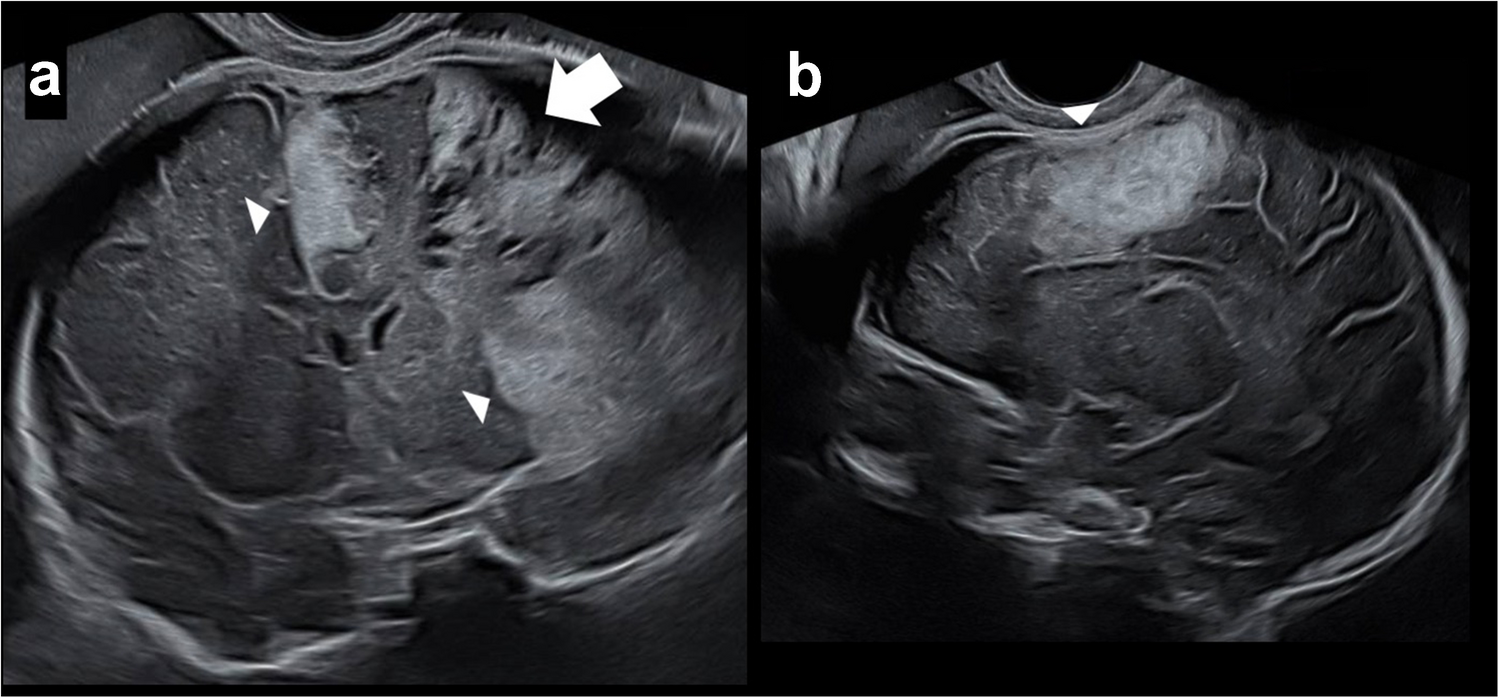
Routine ultrasound (US) at 32 + 4 weeks gestational age revealed a large hyperechogenic area in the left frontal lobe, related to massive hemorrhage, without midline shift. Hemorrhage was also noted above the ipsilateral cerebellum (Fig. 1). A differential diagnosis of parenchymal or extra axial hemorrhage was raised.
Fig. 1
Ultrasound images of the brain in a male fetus at 32 + 4 weeks gestational age demonstrate hemorrhage. a Coronal image shows diffuse parenchyma and extra axial echogenicities, fronto-parietal lobes (arrowhead), with cystic evolution (arrow) consistent with hemorrhages at different stages. b A para-sagittal image shows echogenic parenchyma hemorrhage (arrowhead)
The patient was sent for a fetal MRI, performed the next day, at 32 + 5 weeks gestational age. Imaging revealed a large extra axial collection over the left cerebral hemisphere; a hypointense signal in T2 confirmed as hemorrhage by susceptibility-weighted imaging, with a mild hyperintensity signal in T1. The hemorrhagic fluid collection measured up to 2 cm in maximum depth.
Beneath the hematoma, the underlying brain parenchyma, in the left fronto-parietal-temporal cortex, showed T2 hyperintensity accompanied by diffusion restriction that extended into the left thalamus. Within this parenchymal component area, there were linear, tiny T2 hypointense structures, which suggested the presence of engorged medullary veins. Marked susceptibility to blooming artifacts from hemosiderin deposition was evident in these areas.
Similar signal abnormalities were noted in the frontal interhemispheric region. A focal mass effect with compression of the adjacent parenchyma and a rightward midline shift was also observed (Fig. 2).
Fig. 2
Magnetic resonance images of the brain in a male fetus at 32 + 5 weeks gestational age demonstrate massive subpial hemorrhage. a Coronal T2-weighted image shows extra axial hypointense signal, consistent with a front-parietal lobes hemorrhage (white asterisk). The underlying cortex demonstrates diffuse hyperintense T2 signal (arrow). b Coronal T1-weighted image shows hyperintense signal confirming subacute front-parietal lobes hemorrhage (black asterisk). c Sagittal T2-weighted image shows linear T2 hypointensities within the underlying cortex, suggesting engorged medullary veins (arrowhead). d Axial susceptibility-weighted imaging shows increased susceptibility-blooming-related artefact from hemosiderin in the cortex and the extra axial areas, rendering them indistinguishable on susceptibility images (white asterisk). e Axial diffusion-weighted image shows restricted diffusion in the adjacent parenchyma, differentiating the underlying restrictive cortex from the overlying subpial hematoma. f Axial T2-weighted image shows hypointense subpial hemorrhage (white asterisk), underlying hyperintense cortex (arrow) with a typical “yin-yang” appearance: cortical buckling and patchy cortical and subcortical injury
The characteristic combination of a rounded, egg-shaped subpial hemorrhage with underlying restricted diffusion in the adjacent cortex formed a distinct imaging pattern, resembling the “yin-yang” symbol in Chinese philosophy. On apparent diffusion coefficient maps, true restricted diffusion sharply delineated the cortical ribbon and subcortical white matter adjacent to the subpial hemorrhage, consistent with subpial hemorrhage. Additional infra- and supratentorial hemorrhages were also identified. Maternal and fetal testing, including whole-exome sequencing, as well as tests for coagulopathy and antiphospholipid antibodies, yielded negative results.
Based on these findings, the parents were consulted regarding the risk of abnormal neurologic development associated with the multicompartment hemorrhages. They were offered the option of pregnancy termination, which is permitted under national law in late pregnancy for cases involving a high risk of severe neurodevelopmental impairment.
The pregnancy was terminated at 33 + 1 weeks gestational age due to parental request. Autopsy confirmed the presence of a subpial hemorrhage, as observed on MRI, with no evidence of malformed blood vessels or vascular malformation (Fig. 3).
Fig. 3
Autopsy at 33 + 1 weeks gestational age confirming the subpial hemorrhage seen in fetal magnetic resonance images. a Cerebral hemispheres, superior view. Extensive hemorrhage in the leptomeninges overlying the left hemisphere. b Cerebral hemispheres, coronal section. In frame: Hematoma involving cortex and subcortical zones of the left cerebral hemisphere, associated with dissecting hemorrhages throughout white matter. c Histologic section by hematoxylin and eosin (H&E) staining, taken from the left cerebral hemisphere, in the coronal plane, parallel to the white frame in b (scale bars: 5 mm). In addition to cerebral hematoma and hemorrhages, hemorrhage is seen in the meninges in the superior aspect of the left cerebral hemisphere (arrows) (c). d Masson trichrome stain showing subpial hemorrhage, between the cortex and leptomeninges (scale bars: 50 μm). e Reticulum stain highlighting a subpial hemorrhage separating the cortex and glia limitans (black arrows) from leptomeninges, which contain reticulum fibers (white arrows) (scale bars: 50 μm)
Comments (0)