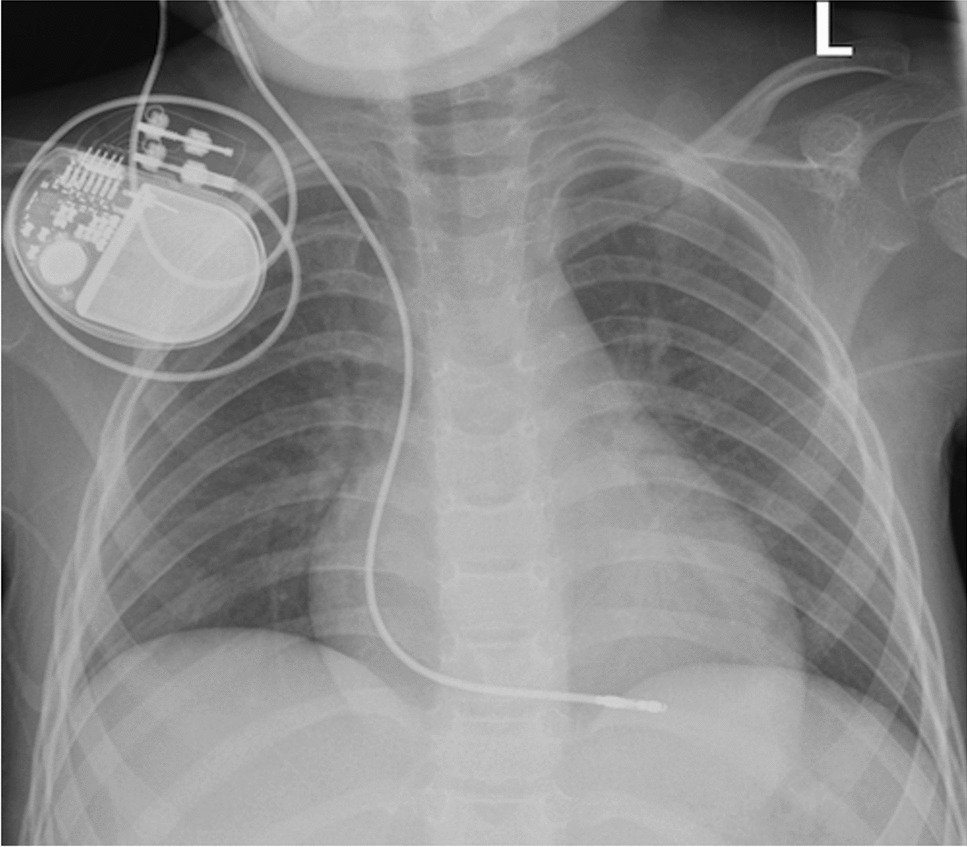
This case demonstrates the feasibility of temporary transvenous pacing with an externalized permanent pacemaker during cardiac MRI in a pediatric patient, aligning with Kakarla et al., who reported safe cardiac MRI in three pediatric myocarditis cases with temporary pacing [1]. Unlike traditional temporary pacemakers (e.g., Model 5392, Medtronic, Minneapolis, MN, USA), which are not MRI-safe due to risks of heating and malfunction, the externalized Assurity MRI™ pacemaker system is MRI-conditional, offering a safer alternative for diagnostic imaging [2, 7]. The externalized Assurity MRI™ pacemaker generator, taped to the skin, and the transvenous lead, positioned in the right ventricle, minimized artifacts compared to traditional pacemakers [2]. Similar to Kakarla et al., our case showed minimal artifacts (<5% of the imaging field), enhancing diagnostic clarity [1]. Cardiac MRI provided critical diagnostic insights, identifying primary conduction system involvement without myocarditis and guiding permanent pacemaker implantation [5, 8].
Compared to echocardiography, which lacks detailed tissue characterization, and computed tomography (CT), which involves ionizing radiation and limited functional assessment, cardiac MRI is superior for pediatric patients requiring repeated imaging [5, 8]. In adults, Fyenbo et al. reported safe MRI with temporary external pacemakers in 44 patients, with minimal artifacts and no adverse events, using VOO mode and strict SAR limits [2]. Our case extends these findings to pediatrics, where smaller anatomies necessitated adjustments, such as precise lead placement and tailored pacing settings, to ensure safety and image quality [3, 6].
Pediatric patients present unique challenges for temporary pacing during MRI, including smaller venous anatomy requiring meticulous lead positioning and higher baseline heart rates necessitating customized pacing parameters [3, 7]. These factors, combined with limited pediatric-specific data on MRI-conditional devices, underscore the need for specialized protocols. Safety measures in our case included VOO pacing, SAR optimization below 2 W/kg, gauze insulation, and continuous real-time monitoring of hemodynamics and surface temperature using fiber-optic sensors, with no RF-induced heating detected [2, 4]. Institutional CIED protocols, involving pre-procedure EP consultations and real-time radiology coordination, ensured rigorous risk management [4, 7]. Unlike Kakarla et al., who used general anesthesia, our patient remained awake, reducing procedural complexity and resource use [1].
However, pediatric-specific data remain limited, and challenges include the need for specialized equipment and multidisciplinary expertise. Future multi-center studies should validate MRI-conditional pacing systems across diverse pediatric populations, while the development of smaller, pediatric-specific devices could further reduce artifacts and enhance safety [6, 7].


Comments (0)