Serosal and soft tissue enhancement is a unique imaging finding that has been reported to mimic pneumoperitoneum [1, 2]. In this study, we found that when assessed by unanimous agreement among three pediatric radiologists, serosal and soft tissue enhancement occurred in 7.1% of infants who underwent abdominal radiographs following cardiac catheterization. While the diagnosis remains somewhat subjective, this rate is higher than what has been suggested by prior case reports and indicates that the phenomenon may be more common than previously appreciated.
Several clinical factors were significantly associated with the presence of serosal and soft tissue enhancement, including lower pre- and post-catheterization creatinine levels, higher total contrast volume administered during the procedure, and higher contrast dose normalized to BSA and weight.
We believe that the contrast volume per BSA and contrast volume per weight are the most significant factors contributing to the development of serosal and soft tissue enhancement. Previous reports suggest that serosal and soft tissue enhancement results from increased lymphatic uptake of contrast agents, likely due to extracellular fluid redistribution driven by elevated hydrostatic pressure. This pressure increase can be further exacerbated by a state of volume overload, causing leakage of contrast and other fluids into the extracellular interstitium [1, 2]. Administering higher total doses of contrast, particularly when adjusted for BSA or weight, may amplify the volume overload, raise hydrostatic pressure, and promote greater retention of contrast within the tissues.
We initially hypothesized that the combination of decreased renal function and higher contrast dose would make the effect of soft tissue and serosal enhancement more pronounced due to decreased renal clearance of the contrast media. However, based on our data, a lower preprocedural creatinine level was associated with this phenomenon. The rationale for this finding is difficult to explain. To explain this finding, we further hypothesized that interventional cardiologists may be purposefully limiting contrast usage in patients with higher creatinine values. This hypothesis was also proven to be incorrect. While patients with a lower creatinine level prior to catheterization did receive more contrast per body surface area, there was no difference between groups in those who developed serosal and soft tissue enhancement and those who did not.
Currently, the diagnosis of serosal and soft tissue enhancement remains subjective. While all three reviewers agreed that serosal and soft tissue enhancement was present in 7.1% of children under 1 year of age who received an abdominal radiograph after cardiac catheterization, the incidence for individual reviewers ranged from 13.9 to 36.7%. This range highlights the subjective nature of the diagnosis and suggests that mild serosal and soft tissue enhancement may be present in more patients than reflected in the final consensus. We believe the reviewer with the highest detection rate may have been more attuned to subtle manifestations of this phenomenon, contributing to their higher identification rate. Given this variability, we recommend that radiologists maintain a high index of suspicion for this finding in infants who have recently undergone cardiac catheterization.
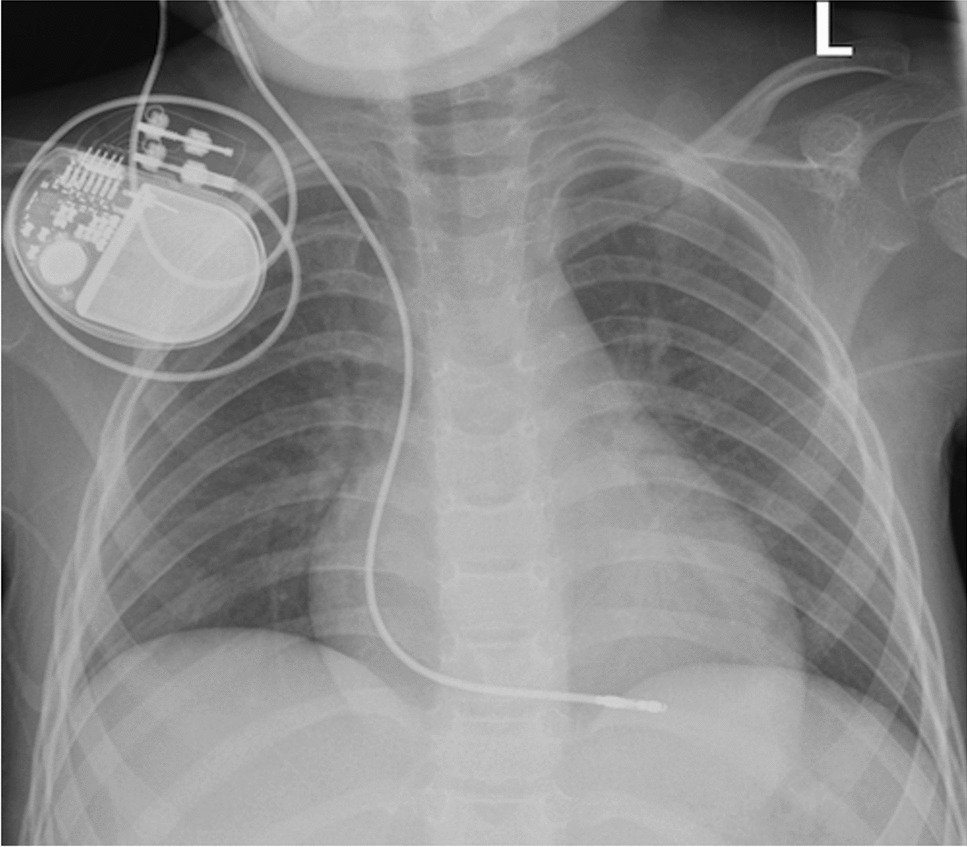
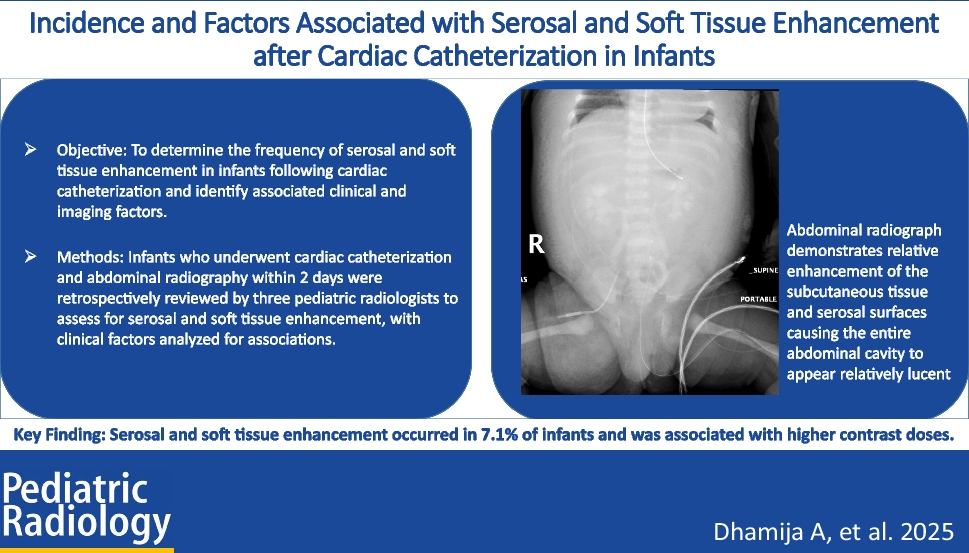
Key findings on abdominal radiograph include high density stranding within the subcutaneous fat, relative lucency of the liver shadow in relation to adjacent soft tissues, and enhancement of the pericardium and peritoneal surfaces. These findings occur while contrast remains visible within the urinary system. While there is little downside to missing subtle instances of this finding on radiograph, knowledge of the entity may help the radiologist explain an unusual appearance of a child’s soft tissues. For example, while we only explored this finding on abdominal radiograph, we have identified differing appearances on chest radiograph and thoracoabdominal CT.
While prior reports have suggested that soft tissue and serosal enhancement can mimic pneumoperitoneum, this diagnosis was not made clinically on any abdominal radiograph in patients determined to have soft tissue and serosal enhancement. However, in one patient, a diagnosis of pneumoperitoneum was made on a preceding chest radiograph and excluded by knowledge of the condition on the abdominal radiograph. Anecdotally, we have observed that this misdiagnosis is more common among trainees and on chest radiographs. The lack of misdiagnosis may reflect knowledge of the condition among our faculty as well as the study’s focus on abdominal radiographs. In patients with recent catheterization and continued imaging concern for pneumoperitoneum, additional imaging with a cross-table lateral or decubitus radiograph could be performed.
Serosal and soft tissue enhancement differs from other types of contrast opacification of soft tissues. Total body opacification of contrast is a distinct phenomenon characterized by widespread distribution of contrast media throughout the body’s tissues and organs following imaging procedures. Soft tissue and serosal enhancement typically occurs in infants after cardiac catheterization and shows a distinctive pattern: contrast enhancement appears in the peritoneum, pericardium, and soft tissues, while sparing solid organs. In contrast, total body opacification shows uniform enhancement across all body regions [3].
Different patterns of contrast enhancement, such as vicarious excretion, organ enhancement, and contrast retention, further illustrate the complexity of contrast media distribution. Vicarious excretion involves the non-renal excretion of contrast media, often seen in cases of renal impairment, leading to unusual enhancement in the liver and gastrointestinal tract [4,5,6]. Organ enhancement refers to specific uptake by various organs, indicating underlying pathologies like tumors or inflammation. Contrast retention occurs when the contrast media remains in the body tissues for extended periods due to impaired renal function, posing potential toxicity [7]. These patterns highlight the importance of understanding contrast media distribution for accurate diagnosis and patient management.
In pediatric imaging, the dosage of contrast media varies significantly between cardiac catheterization and CT scans. Cardiac catheterization generally involves higher total doses of contrast agents (1 mL/kg/bolus run) due to the need for detailed visualization of the heart and major vessels, which increases the risk of serosal and soft tissue enhancement and related phenomena. Contrast-enhanced CT scans typically use lower doses of contrast media (1-2 mL/kg/per scan) thereby reducing the likelihood of extensive contrast enhancement. In our study, patients who developed serosal and soft tissue enhancement received higher contrast doses during cardiac catheterization (7.56±4.20 mL/kg) compared to those without serosal and soft tissue enhancement (4.77±3.27 mL/kg), supporting the association between higher contrast exposure and the development of this phenomenon.
In evaluating cardiac physiology, we focused on the function of the ventricle receiving systemic venous return, based on the hypothesis that impaired ventricular function could reduce contrast clearance and contribute to the development of serosal and soft tissue enhancement. However, this hypothesis was not supported by our data, as no association was found between ventricular function and the presence of serosal and soft tissue enhancement. This finding is not unexpected, as other cardiac factors may play a role in the development of serosal and soft tissue enhancement, such as end-diastolic pressure and atrioventricular valve regurgitation. These variables represent important areas for future investigation.
There are several limitations of this study. Besides the primary limitation of identifying a subjective finding, the other main limitation is a potential referral bias. Of nearly 1800 patients who underwent cardiac catheterization, only approximately 1 in 6 underwent subsequent abdominal radiograph within the first 2 days after the procedure. It is possible that these patients were inherently different than the patients who did not receive abdominal radiograph. This difference may affect the frequency of diagnosis or the underlying risk factors. Additionally, it is possible that the inclusion time frame of a radiograph performed within 2 days of cardiac catheterization is not appropriate. A different time frame could influence the overall incidence of the finding. Finally, cardiac function was not determined for most patients. This limits our ability to determine if serosal and soft tissue enhancement is associated with ventricular function. However, there was no difference in left ventricular fractional shortening between patients with or without serosal and soft tissue enhancement.


Comments (0)