
Remember me
Our data indicate that medical and nursing students viewed the SS of the LHoL as a positive learning experience. They emphasized its necessity, value, and utility for their future practice, recognizing LHoL as a key aspect of their clinical reality.
Moreover, several of the themes and sub-themes highlighted by the students closely align with the educational objectives established in the Spanish national guidelines for undergraduate training in Medicine and Nursing [13, 14]. They are also consistent with the accreditation standards defined for PC professionals [15, 16] as well as with the recommendations issued by national and international organizations in the field of PC [17, 18]. From both degree perspectives, this training fosters the development of essential clinical competencies such as terminal patient assessment, holistic care, breaking bad news, symptom management, and clinical decision-making in complex scenarios. Additionally, it strengthens key transversal skills including teamwork, empathy, and emotional sensitivity to the suffering and needs of patients and their families.
Both student groups highlighted that the scenario underscored the significance of their role as healthcare professionals and the impact they can have on the patient and family during difficult times. These findings are significant because death is frequently perceived as a failure in medical literature [19], although end-of-life care is part of the ethical codes of medicine and nursing, including patient and family support, limiting diagnostic actions, palliative sedation, etc. [20]
The study results support the notion that simulation is an effective pedagogical strategy for applying theoretical knowledge in a controlled, authentic environment [8, 21,22,23,24,25]. Specifically, it demonstrates that simulation is feasible and beneficial for teaching end-of-life care.
Students recognized that the content of this SS was relevant to genuinely delicate situations, such as the LHoL and death. This finding aligns with existing literature [25, 26], which identifies conversations and support for patients and their families during these final hours as particularly challenging. Teaching care in LHoL is rarely included in medical curricula. Only one study with four medical students involved a hybrid simulation of a patient with terminal lung cancer has been found [24]. Pre- and post-test results indicated improved attitudes towards caring for terminal patients and their families, suggesting that this approach effectively enhances attitudes in the absence of experiential learning. In nursing education, there is slightly more coverage of the topic, with several studies indicating that death scenarios are seen as positive and useful learning experiences [25, 27,28,29]. These studies emphasize the importance of the support and care nurses should provide to patients and their families, highlighting the greater emphasis placed in nursing education on addressing both patient and family needs. This is consistent with the findings of our study, in which only nursing students referred to the reaffirmation the SS provided in recognizing the value of being present for the patient and offering support to families—an aspect not mentioned by medical students.
Globally, the limited number of studies on teaching care in the LHoL may be attributed to death being a taboo subject both socially and within healthcare contexts [19]. In addition, although cultural norms significantly influence how death is perceived, communicated, and managed, particularly in increasingly multicultural societies, this simulated scenario was intentionally designed to remain culturally neutral. No specific reference was made to religious beliefs, familial traditions, or cultural rituals. The primary aim was to expose students to a general end-of-life situation, emphasizing the recognition of universal signs and symptoms of dying, as well as the communication of this process in a respectful and professional manner. This neutral approach enhances its potential transferability across diverse educational settings. Any necessary adjustments for local implementation would mostly involve communication styles or cultural values that could be discussed during the debriefing phase, rather than the core structure of the scenario itself. In fact, the workshop has been translated into English and included in a European project (E-Learning on Palliative Care for International Students, ELPIS) [30], in which its content and structure were reviewed and endorsed by partners from six different countries. This reinforces the scenario’s relevance and applicability in diverse cultural and educational contexts.
Searches for training on death and dying predominantly yield references to courses on cardiopulmonary resuscitation and emergency care [31]. While some simulations focus on delivering bad news to families following unexpected deaths, this represents only a partial view of the broader realities of death within the healthcare system. The SS in the LHoL carried out in this study offers an alternative perspective on death and highlights the value, usefulness, necessity, and positive impact according to students of such an intervention. Both nursing and medical students emphasized that learning to address the needs and emotions of patients and families, beyond vital signs, is crucial for understanding their responsibilities [29].
Students acknowledged that they will encounter such delicate situations in their careers and found the SS a valuable learning experience. They appreciated the clinical guidance it provided, including recognizing physiological signs of dying and prioritizing comfort, rather than solely focusing on communication skills, as is commonly emphasized in the literature [31,32,33]. Focusing on knowledge beyond theoretical content, only medical students specifically highlighted the value of the workshop in helping them to gain essential emotional management. This aspect of emotional self-awareness was not explicitly mentioned by nursing students, whose reflections were more focused on responding to the needs of patients and their families. This difference may be attributed to the intense emotional burden experienced by medical students, as many were confronting, for the first time, a highly sensitive situation such as the death of a patient and the task of breaking the news to their family.
Students considered the realism of the SS critical for accurately experiencing and handling the situation. The use of standardized actors as both patient and family member, rather than the typical hybrid scenario with a manikin as a patient and standardized actor as a family member [34,35,36], was considered beneficial. In another study, nursing students have noted that hybrid scenarios lack realism due to the limited interaction with manikins [34]. In contrast, in our study, the use of standardized actors throughout the SS was noted to have a significant impact, eliciting emotions that encouraged reflection on both theoretical-practical and introspective levels.
This SS could also offer an opportunity for interprofessional team building, a crucial competency in LHoL care [35, 36]. This aspect was highlighted solely by medical students, who found the assistance of nurses during the SS to be highly valuable and emphasized the importance of teamwork. This discrepancy may be attributed to the presence of a nurse in the medicine scenarios, whereas nursing scenarios did not include a presential doctor.
The realism of the SS also facilitated introspection regarding students’ emotional responses and their management. Both medical and nursing students acknowledged that the simulation evoked strong emotions, which is an inherent aspect of caring for patients in the LHoL who are often unconscious and supporting their family as death approaches [37,38,39,40].
During the debriefing, medical and nursing students requested strategies for managing emotions, focusing not only on how to deal with those of family members but also primarily on their own. This reflects an initial step towards professional self-awareness, which is increasingly recognized in the literature as essential for developing self-care throughout a clinical career [41, 42]. However, further research is needed to validate and explore the effectiveness of simulation in teaching and reflecting on professional self-care.
The introspection also involved their roles as healthcare students, who felt like authentic professionals during the SS. They deeply contemplated their professional roles as doctors/nurses, gaining a true understanding of their responsibilities, an aspect that has not been found in any other article. For nursing students, it was a confirmation of their role in contributing to patients and families [43, 44], while for doctors, it was more about discovering the human aspect of their profession. They recognized they are humans, not just providers of medical techniques, highlighting the importance of a holistic, empathetic approach to patient care. This underscores the current dehumanization in medicine [19, 45].
This reflective reasoning in Medical and Nursing students suggests that simulations can aid in developing attitudes, not just theoretical and practical skills [29]. It may also contribute to the hidden curriculum, but further studies are needed to confirm this.
The limitations of this study include that the research was conducted in one university, which may limit the generalizability of the findings. A 50–67% response rate is good for a one-time contact study. Higher rates might have been achieved with follow-up reminders. Incorporating member checking could help validate the interpretations and enhance the trustworthiness of the findings. While analyzing the quotes from active students and observers separately could have strengthened the results, doing so might have compromised participant anonymity. Medicine students reported shifts in their professional role and perspective. Quantitative assessments of these changes would be valuable. Furthermore, future research should incorporate longitudinal studies assessing the impact of this kind of scenario in the daily clinical practice. It would be interesting to explore the potential of a shared SS of this type to promote interprofessional team building during the LHoL of a patient.
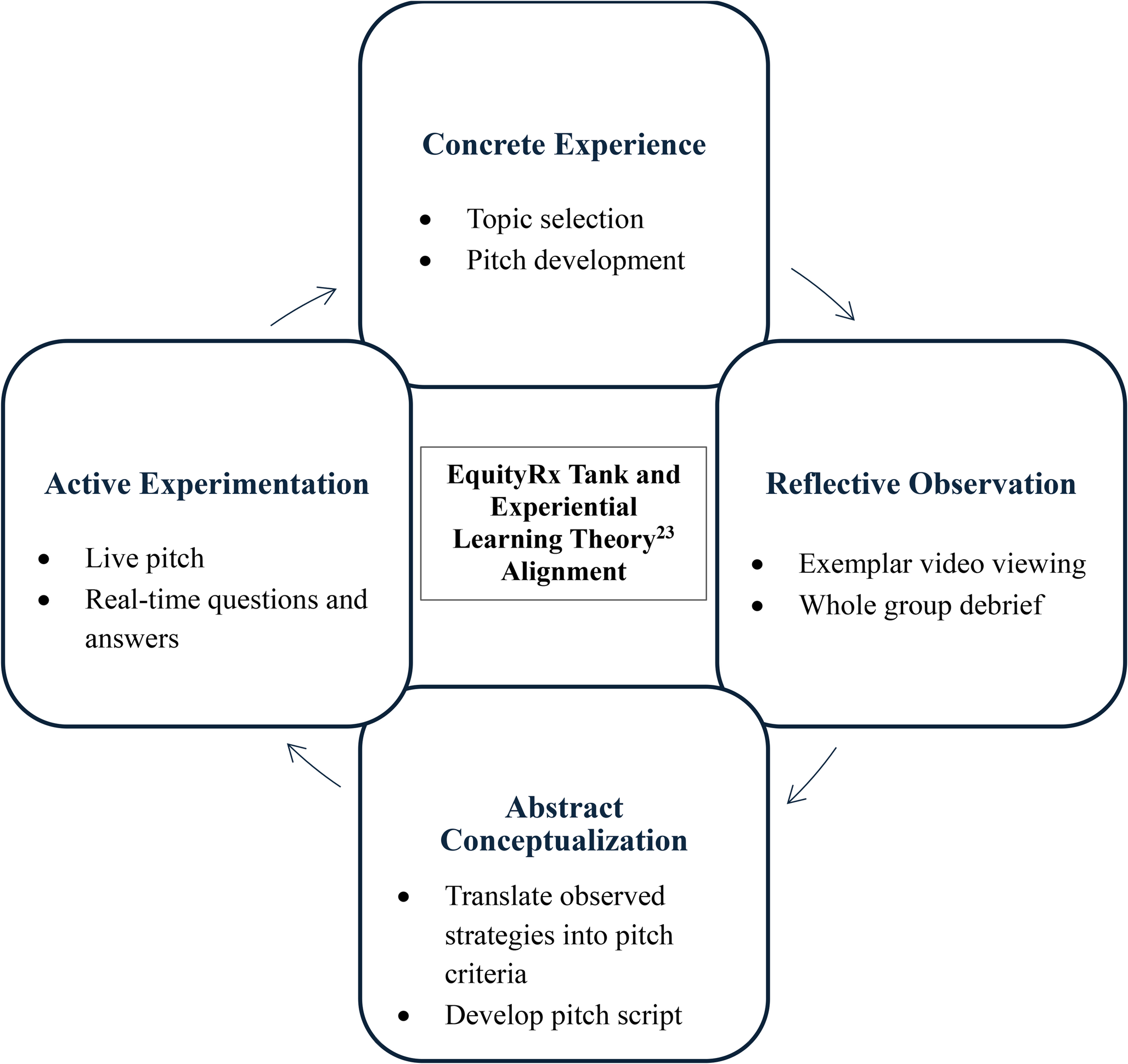
In sum, Medicine and Nursing students perceived the SS of LHoL with standardized patients as a realistic, positive, and safe learning experience. It allowed them to manage both their own professional self-awareness and patients’ emotions, provided practical tools for navigating sensitive clinical situations, provided useful knowledge for sensitive situations (practical guidelines), and prompted deep introspection about their professional role (Fig. 2).
Fig. 2
Conceptual flowchart representing the learning process experienced by healthcare students during SS of LHoL. On the left side, the diagram illustrates how the SS fosters experiential learning, which elicits emotions and prompts individual reflection. On the right side, arrows show the learning outcomes—both cognitive and attitudinal—derived from this process, ultimately contributing to professional growth and the application of theoretical knowledge in practice. The words included within each box represent word clouds extracted from students’ qualitative responses; the size of each word reflects its frequency in the comments
The insights and competencies reflected by students through this SS are closely aligned not only with the educational objectives of PC, but also with broader learning goals in Medicine and Nursing degrees and accreditation standards. This alignment reinforces the value of the SS as an effective pedagogical tool for fostering essential clinical competencies and transversal skills such as symptom recognition, communication, and holistic care.
Given its educational relevance and clinically oriented design, this SS could be adapted for use in other international contexts, though it remains essential to consider the cultural factors that influence how death is perceived and managed across societies.
A valuable next step would be a longitudinal study using a mixed-methods approach to combine quantitative and qualitative data, aimed at evaluating the long-term impact of this SS on clinical performance and emotional resilience.
Comments (0)