
Remember me
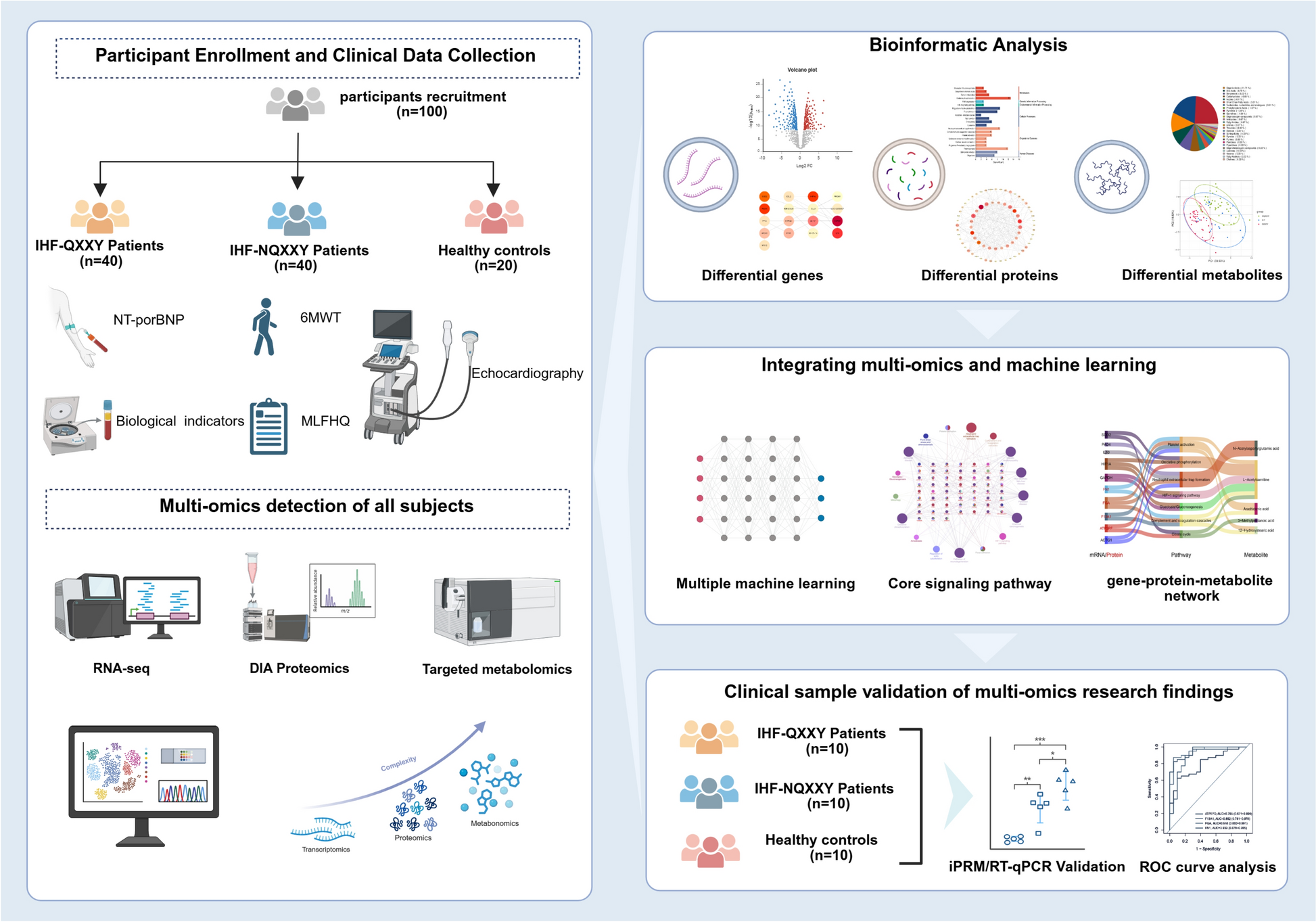
From June 2022 to January 2023, we recruited 100 eligible participants from the cardiovascular outpatient clinic of the First Affiliated Hospital of Henan University of Chinese Medicine and surrounding communities, comprising 40 IHF patients with QXXY Syndrome (IHF-QXXY), 40 with NQXXY Syndrome (IHF-NQXXY), and 20 healthy controls (HC). The demographic and clinical biochemical characteristics of the participants are presented in Table 1. Age, sex, DBP, and BMI did not differ significantly among the IHF-QXXY, IHF-NQXXY, and HC groups (P > 0.05). However, significant differences were observed in SBP, blood lipid and glucose levels, as well as PT and APTT, reflecting glucose-lipid metabolism disorders and coagulation abnormalities in IHF patients. The IHF-QXXY and IHF-NQXXY groups showed no statistically significant differences in age, sex, DBP, BMI, history of hypertension, hyperlipidemia, diabetes, or laboratory findings. Notably, compared with the IHF-NQXXY group, the IHF-QXXY group had a greater proportion of patients with NT-proBNP levels below 1000 pg/ml and NYHA functional class I–II. Furthermore, the IHF-QXXY group demonstrated a higher LVEF (41.00% vs. 35.28%, P = 0.001), longer 6WMD (371.37 m vs. 312.23 m, P = 0.014), and lower MLHFQ scores (44.98 vs. 52.93, P = 0.019). These differences indicate that QXXY Syndrome patients are in a relatively stable phase of IHF, whereas those with NQXXY Syndrome may be experiencing disease progression (Table 2).
Table 1 Baseline demographic and biochemical characteristicsTable 2 The difference of cardiac function indexes between IHF-QXXY group and IHF-NQXXY groupBiological characteristics of IHF-QXXY syndromeTo elucidate the biological characteristics of IHF-QXXY syndrome, we assessed 16 indicators associated with energy metabolism, endothelial function, inflammation, coagulation, and neutrophil extracellular traps (NETs) formation. The assessed indicators included ATP, acetyl-CoA, ET-1, NO, ICAM-1, VCAM-1, TNF-α, IL-1β, IL-6, PGI2, TAT, TXA2, MPO, cfDNA, Cit-H3, and NE. Our results showed a significant decrease in energy metabolism indicators in IHF-QXXY syndrome patients (Fig. 1A–B), with ATP levels decreasing by an average of 16.36 nmol/ml (P < 0.05) and acetyl-CoA by 2.038 ng/ml (P < 0.05) compared to the HC group. Compared to IHF-FXXY syndrome, ATP and acetyl-CoA levels showed no significant differences (P > 0.05). Endothelial function indicators were significantly altered in IHF-QXXY syndrome patients (Fig. 1C–D), with ET-1 levels increasing by 2.764 pg/ml (P < 0.01) and NO levels decreasing by 68.10 μmol/L (P < 0.01) compared to the HC group. ET-1 and NO levels did not significantly differ between IHF-QXXY and IHF-FXXY syndrome (P > 0.05). Patients with IHF-QXXY syndrome exhibited significantly elevated inflammatory response markers (Fig. 1E–I). Compared to the HC group, ICAM-1 levels increased by 5.541 ng/ml (P = 0.005), VCAM-1 by 110.6 ng/ml (P < 0.05), TNF-α by 22.22 pg/ml (P < 0.05), IL-1β by 1.731 pg/ml (P < 0.05), and IL-6 by 3.193 pg/ml (P < 0.05). Compared to the IHF-NQXXY syndrome group, VCAM-1 levels were further elevated (P < 0.05), whereas other inflammatory markers showed no significant differences (P > 0.05). These findings indicate that patients with IHF QXXY syndrome experience a marked chronic inflammatory response. Additionally, patients with IHF-QXXY syndrome displayed abnormal coagulation function markers (Fig. 1J–L). Compared to the healthy group, PGI2 levels decreased by 294.2 pg/ml (P < 0.05), TXA2 levels increased by 24.05 pg/ml (P < 0.05), and TAT levels showed an upward trend. Patients with IHF-QXXY syndrome exhibited significantly elevated NETs-related markers (Fig. 1M–P). Compared to the HC group, cfDNA concentration increased by an average of 3.533 ng/ml (P < 0.05), Cit-H3 by 30.02 pg/ml (P < 0.05), NE by 17.99 ng/ml (P < 0.05), and MPO showed a slight upward trend (P < 0.05). These findings suggest that NETs formation plays a role in the progression of IHF-QXXY syndrome.
Fig. 1
Biological characteristics of IHF-QXXY syndrome. A The level of ATP in each group was detected by ELISA kit. B The level of Acetyl-CoA in each group was detected by ELISA kit. C The level of ET-1 in each group was detected by ELISA kit. D The level of NO in each group was detected by ELISA kit. E The level of ICAM-1 in each group was detected by ELISA kit. F The level of VCAM-1 in each group was detected by ELISA kit. G The level of TNF-α in each group was detected by ELISA kit. H The level of IL-1β in each group was detected by ELISA kit. I The level of IL-6 in each group was detected by ELISA kit. J The level of PGI2 in each group was detected by ELISA kit. K The level of TAT in each group was detected by ELISA kit. L The level of TXA2 in each group was detected by ELISA kit. M The level of MPO in each group was detected by ELISA kit. N The level of cfDNA in each group was detected by ELISA kit. O The level of Cit-H3 in each group was detected by ELISA kit. P The level of NE in each group was detected by ELISA kit. *P < 0.05; ** P < 0.01; *** P < 0.001; **** P < 0.0001
Transcriptomic characteristics of IHF-QXXY syndromeBlood transcriptomes from the HC, IHF-QXXY, and IHF-NQXXY groups were sequenced using the Illumina high-throughput platform. PCA demonstrated clear separations among the HC, IHF-QXXY, and IHF-NQXXY groups (Fig. 2A). The DESeq2 software was used for intergroup analysis of DEGs(|log2FC|≥ 1, P < 0.05). The IHF-QXXY vs. HC comparison revealed 318 DEGs, with 115 upregulated and 203 downregulated genes (Fig. 2B). The IHF-NQXXY vs. HC comparison identified 369 DEGs, with 166 upregulated and 203 downregulated genes (Fig. 2C). Venn diagram analysis (Fig. 2D) identified 241 DEGs unique to QXXY syndrome, comprising 121 upregulated and 120 downregulated mRNAs. Using clusterProfiler (version 4.12.0), pathway enrichment analysis of QXXY syndrome-specific DEGs revealed significant enrichment in immune-inflammatory pathways, including NETs Formation, Chemokine Signaling, NF-kappa B Signaling, and B Cell Receptor Signaling (Fig. 2E). To explore key genes in QXXY syndrome, a gene–gene interaction network was constructed and optimized in Cytoscape using STRING data, comprising 98 nodes and 239 edges (Fig. 2F). CytoHubba analysis integrating MCC, MNC, and Degree algorithms identified 17 hub DEGs with high centrality and betweenness (Fig. 2G). Machine learning analysis of the 17 hub DEGs identified 13 feature genes by LASSO, 8 by SVM-RFE, and 8 by RF (Fig. 2H–J). The intersection of these methods revealed six candidate biomarkers (HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH) (Table S4). ROC analysis showed that the AUC values for HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH ranged from 0.627 to 0.693 (Fig. 2K). The combined diagnostic AUC reached 0.863 (95% CI: 0.754–0.948), suggesting strong diagnostic potential and reliability (Fig. 2L).
Fig. 2
Transcriptomic characteristics of IHF-QXXY syndrome. A Classification results of HC, IHF-QXXY, and IHF-NQXXY groups based on PCA score plot. B The volcano plots of DEGs between IHF-QXXY and HC group. C The volcano plots of DEGs between IHF-NQXXY and HC group. D Venn diagram of specific DEGs to IHF-QXXY syndrome. E Pathway enrichment of specific DEGs to IHF-QXXY syndrome. F PPI network analysis of specific DEGs to IHF-QXXY syndrome. G The top 17 nodes of the PPI network identified by the MCC, MNC, and Degree algorithms. H LASSO analysis screening of feature genes. I SVM-RFE algorithm screening of feature genes. J RF algorithm screening of feature genes. K ROC curve of HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH. L Combined diagnostic ROC curves of feature genes
Proteomic characteristics of IHF-QXXY syndromeNext, we conducted DIA-based proteomics analysis. The results of PLS-DA revealed clear sample dispersion between different groups, while samples within the same group clustered together (Fig. 3A). A total of 759 DEPs were obtained in IHF-QXXY vs. HC group and IHF-NQXXY vs. HC group. A total of 211 DEPs were identified between the QXXY and HC groups, with 100 upregulated and 111 downregulated (Fig. 3B). Between the NQXXY and HC groups, 639 DEPs were identified, including 356 upregulated and 283 downregulated (Fig. 3C). A Venn diagram intersection analysis identified 120 differential proteins specific to QXXY syndrome, with 41 upregulated DEPs and 79 downregulated DEPs (Fig. 3D). KEGG pathway enrichment analysis was conducted on the specific DEPs of QXXY syndrome to identify the key biochemical and signaling pathways involved. The results revealed that these DEPs were primarily associated with NETs, complement and coagulation cascades, platelet activation, glycolysis/gluconeogenesis, and the HIF-1 signaling pathway (Fig. 3E). The PPI network of specific DEPs for QXXY syndrome was constructed using Cytoscape, as shown in Fig. 3F, with 105 nodes and 239 edges. Using multiple algorithms based on the CytoHubba plugin, an intersection was performed, identifying 19 DEPs with high centrality and betweenness centrality (Fig. 3G). Additionally, LASSO, SVM-RFE, and RF algorithms identified 5, 13, and 7 feature proteins, respectively (Fig. 3H–J, Table S5). The intersection of the feature proteins from these algorithms is presented in a Venn diagram, identifying candidate biomarkers FGA, FN1, F13A1, and ATP5PF. ROC analysis showed that the AUC values for FGA, FN1, F13A1, and ATP5PF were 0.948, 0.939, 0.892, and 0.787, respectively Fig. 3K). The combined diagnostic performance of these biomarkers yielded an AUC of 0.956 (95% CI: 0.896–0.998), underscoring their diagnostic accuracy and reliability in assessing QXXY syndrome (Fig. 3L).
Fig. 3
Proteomic characteristics of IHF-QXXY syndrome. A Classification results of HC, IHF-QXXY, and IHF-NQXXY groups based on PLS-DA score plot. B The volcano plots of DEPs between IHF-QXXY and HC group. C The volcano plots of DEPs between IHF-NQXXY and HC group. D Venn diagram of specific DPGs to IHF-QXXY syndrome. E Pathway enrichment of specific DEPs to IHF-QXXY syndrome. F PPI network analysis of specific DEPs to IHF-QXXY syndrome. G The top 19 nodes of the PPI network identified by the MCC, MNC, and Degree algorithms. H LASSO analysis screening of feature proteins. I SVM-RFE algorithm screening of feature proteins. J RF algorithm screening of feature proteins. K ROC curve of FGA, FN1, F13A1, and ATP5PF. L Combined diagnostic ROC curves of feature proteins
Metabolomic characteristics of IHF-QXXY syndromeTargeted metabolite identification and quantification were conducted on blood samples from the HC, IHF-QXXY, and IHF-NQXXY groups using multiple reaction monitoring. In total, 299 metabolites were identified and classified into 26 categories, with the predominant groups including organic acids (11.71%), bile acids (8.70%), benzenoids (8.03%), carbohydrates (6.69%), indoles (4.01%), short-chain fatty acids (4.01%), nucleosides, nucleotides, and analogues (3.01%), phenylpropionic acids (1.67%), pyridines (1.34%), quinolines (1.00%), and fatty amides (0.67%), as shown in Fig. 4A. Using the PLS-DA model, we established the relationship between metabolite expression levels and sample groups, demonstrating significant differences among the HP, QXXY, and NQXXY groups (Fig. 4B). Using the criteria of VIP > 1, P < 0.05, and FC > 1.2 or FC < 0.83, we identified 150 endogenous DMs in plasma, including 73 DMs between the QXXY and HC groups, 82 DMs between the NQXXY and HC groups (Fig. 4C, D), and 20 DMs specific to QXXY syndrome (Fig. 4E). Functional enrichment analysis (Fig. 4F) indicated that the DMs specific to QXXY syndrome were predominantly enriched in pathways related to arachidonic acid metabolism, platelet activation, biosynthesis of unsaturated fatty acids, alanine, aspartate, and glutamate metabolism, as well as valine, leucine, and isoleucine degradation. ROC diagnostic analysis demonstrated that the AUC values for 3-methylpentanoic acid, arachidonic acid, N-acetylaspartylglutamic acid (NAAG), L-acetylcarnitine, and 12-hydroxystearic acid were 0.798, 0.696, 0.649, 0.694, and 0.653, respectively (Fig. 4G). When combined, these metabolites exhibited an enhanced diagnostic performance with an AUC of 0.866 (95% CI: 0.767–0.950), suggesting their potential as key metabolic markers for QXXY syndrome (Fig. 4H).
Fig. 4
Metabolomic characteristics of IHF-QXXY syndrome. A Pie chart of identified metabolites. B PLS-DA score plot of the HC, IHF-QXXY, and IHF-NQXXY groups. C The volcano plots of DMs between IHF-QXXY and HC group. D The volcano plots of DMs between IHF-NQXXY and HC group. E Venn diagram of specific DMs to IHF-QXXY syndrome. F Pathway enrichment of specific DMs to IHF-QXXY syndrome. G ROC curve of 3-methylpentanoic acid, arachidonic acid, N-acetylaspartylglutamic acid, L-acetylcarnitine, and 12-hydroxystearic acid. H Combined diagnostic ROC curves of Key metabolites
Integrated analysis of DEGs, DEPs, and DMsThe biological foundation of QXXY syndrome was elucidated through the integration of transcriptomics, proteomics, and metabolomics data. Initially, KEGG pathway enrichment analysis was performed using ClueGO and CluePedia, based on RNA-seq and proteomics data, with statistical significance defined as P < 0.05. KEGG enrichment analysis showed that the pathways that had significant influence were Neutrophil extracellular trap formation, Platelet activation, Complement and coagulation cascades, HIF-1 signaling pathway, Glycolysis/Gluconeogenesis, and oxidative phosphorylation (Fig. 5A). Within the KEGG pathway network, we identified candidate biomarkers such as HIF-1α, IL10, PAD4, ACTG1, SOD2, GAPDH, FGA, FN1, F13A1, and ATP5PF, all of which interact with other genes. Subsequently, the DEGs, DEPs, and DMs associated with QXXY syndrome were mapped to the KEGG pathway database to uncover shared pathway information and identify key biochemical and signaling pathways. Results revealed that Platelet Activation, NETs, HIF-1 Signaling, Citrate Cycle, Valine, Leucine, and Isoleucine Degradation, and Alanine, Aspartate, and Glutamate Metabolism were the most enriched pathways in DEGs, DEPs, and DMs (Fig. 5B). Additionally, candidate biomarkers played pivotal roles within these pathways. Furthermore, we found that DEGs, and DEPs were predominantly upregulated in the HIF-1 Signaling Pathway, Glycolysis/Gluconeogenesis, and NETs, whereas they were mostly downregulated in Platelet Activation. Due to energy metabolism disorders, Valine, Leucine, and Isoleucine Degradation as well as Alanine, Aspartate, and Glutamate Metabolism were upregulated, whereas the Citrate Cycle exhibited a downregulation trend. Therefore, we constructed a “gene-protein-pathway-metabolite” network for QXXY syndrome. The multi-omics network of QXXY syndrome comprises six mRNAs, four proteins, five metabolites, and seven pathways (Fig. 5C). We propose that QXXY syndrome’s biological basis is closely linked to energy metabolism dysregulation, immune-inflammatory responses, and coagulation abnormalities mediated by pathways such as NETs, Platelet Activation, Complement and Coagulation Cascades, HIF-1 Signaling, Glycolysis/Gluconeogenesis, Citrate Cycle, and Oxidative Phosphorylation.
Fig. 5
Integrated analysis of multi-omics experiments. A ClueGO analysis of KEGG pathway enrichment. B Enrichment analysis of KEGG pathway shared by DEGs, DEPs, and DMs. C IHF-QXXY syndrome “gene-protein-metabolite” network
RT-qPCR validationWe further validated the expression of the feature genes identified in transcriptomics. We randomly selected blood samples from 10 patients in each of the HP, QXXY, and FQXXY groups and used RT-qPCR to validate the expression levels of HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH. The results showed that the expression levels of HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH were higher in heart failure patients with Qi deficiency and blood stasis syndrome compared to the HP group. The ROC curve was used to assess HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH (Fig. 6A–F). The AUC values for the molecules were as follows: ACTG1 [0.915, 95% CI (0.765, 1.000)] > HIF-1α [0.910, 95% CI (0.750, 1.000)] > PAD4 [0.890, 95% CI (0.720, 1.000)] > SOD2 [0.820, 95% CI (0.610, 0.980)] > GAPDH [0.830, 95% CI (0.600, 0.980)] > IL10 [0.800, 95% CI (0.580, 0.970)] (Fig. 6H).
Fig. 6
The expression of candidate markers was verified by RT-qPCR and iPRM. A The mRNA expression of ACTG1. B The mRNA expression of HIF-1α. C The mRNA expression of PAD4. D The mRNA expression of SOD2. E The mRNA expression of GAPDH. F The mRNA expression of IL-10. G iPRM validation of key DEPs. H Validated ROC curves of HIF-1α, IL10, PAD4, ACTG1, SOD2, and GAPDH. I Validated ROC curve of FGA, FN1, F13A1, and ATP5PF. *P < 0.05; **P < 0.01
iPRM validationTo further validate the feature proteins identified in the discovery phase, iPRM-targeted proteomics was used to verify the feature proteins FGA, FN1, F13A1, and ATP5PF4 in QXXY syndrome. Among the detected proteins, the key target proteins FGA, FN1, and F13A1 in the platelet activation pathway were significantly downregulated, while the key protein ATP5PF4 in the energy metabolism pathway also showed significant downregulation, as shown in Fig. 6G. ROC curve analysis was conducted to evaluate the diagnostic performance of FGA, FN1, F13A1, and ATP5PF4. The AUC values for these proteins were as follows: F13A1 [0.980, 95% CI (0.910, 1.000)] > FGA [0.940, 95% CI (0.790, 1.000)] > FN1 [0.810, 95% CI (0.580, 0.980)] > ATP5PF4 [0.760, 95% CI (0.500, 1.000)], demonstrating high diagnostic performance and further validating their reliability as feature proteins for IHF-QXXY syndrome (Fig. 6I).
Comments (0)