
Remember me
The analysis identified the most suitable surgical applications for exoscopic surgery within head and neck procedures, specifically for otologic, oncologic, and cervical soft tissue surgeries. From an ergonomic perspective, exoscopic surgery could provide a significant advantage for these types of procedures, where surgeons and assistants often find themselves maintaining a flexed neck posture during traditional surgeries.
Exosopic surgery was found to be particularly beneficial in parotid surgery, where enhanced visualization can improve surgical precision for both the primary surgeon and the assisting surgeon. A major risk in parotid gland surgery is injury to the facial nerve, so these procedures are routinely performed with neurophysiologic monitoring and direct optical assessment by an assisting surgeon at our institution. The assistant typically stands opposite the primary surgeon and observes the patient’s sterilely draped face for any involuntary movements, indicating nerve stimulation. However, this position offers limited direct visualization of the surgical site. Exoscopic visualization, displayed on multiple monitors or through the HMDmd, could enhance the assistant’s view of the surgical field, possibly allowing for better intraoperative participation and improved surgical training opportunities.
Another promising application is microvascular soft tissue surgery, particularly for anastomotic suturing in free flap reconstruction. Most commercially available surgical microscopes are designed primarily for neurosurgery, hand surgery, ophthalmology, or otologic surgery, where the line of sight is either directly overhead (as in neurosurgery and ophthalmology) or laterally oriented for a single surgeon (as in otologic procedures). However, microvascular anastomoses in cervical soft tissue reconstructions are often performed by two surgeons, an operator and an assistant, using dual opposing ocular tubes on the microscope. The main limitation in these cases is that the microscope is positioned obliquely lateral to the cervical soft tissues, and the ocular tube of the assistant sitting opposite of the surgeon is often too short for comfortable viewing and manipulation.
This limitation is addressed by the exoscope, which allows both the primary surgeon and assistant to view the surgical field simultaneously on high-resolution 3D monitors or through head-mounted displays. As a result, both team members can maintain ergonomic working positions independent of physical access to oculars, which enhances cooperation, precision, and overall surgical flow in microvascular procedures.
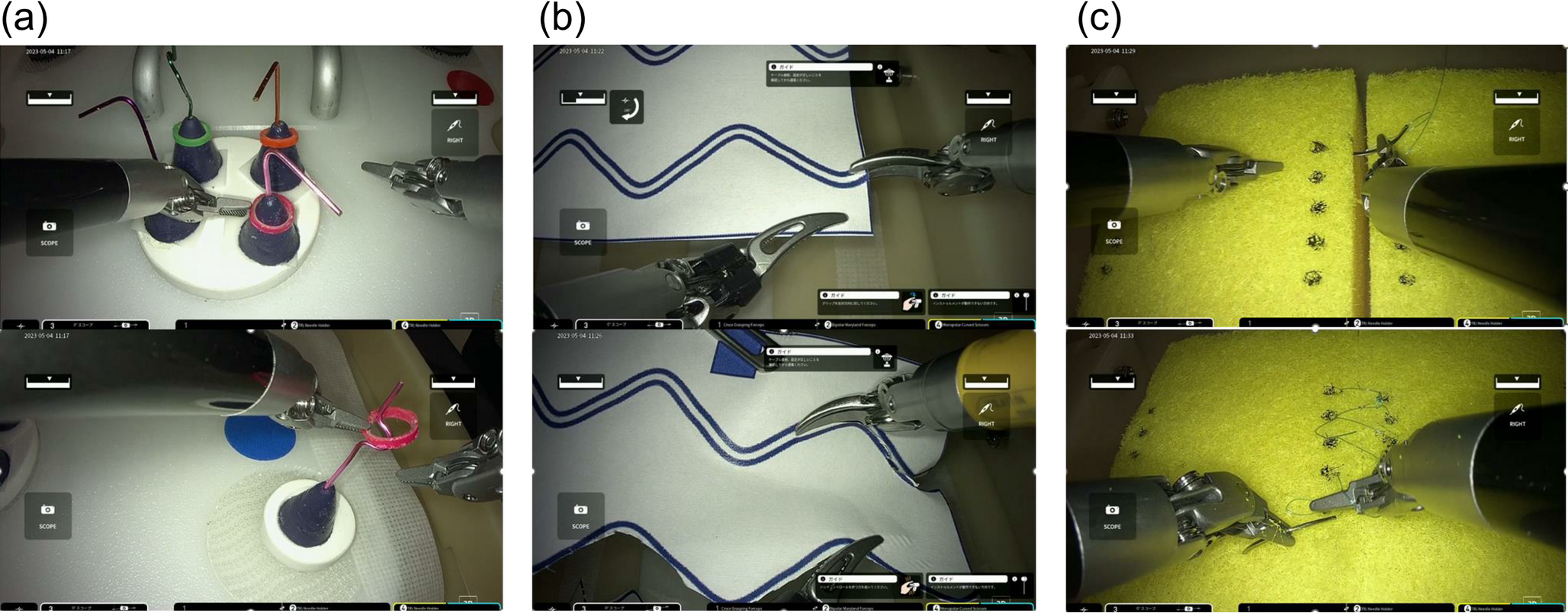
Conduction of the surgeries with exoscopic approachFollowing the identification of these surgical applications, a total of 11 exoscopic/hybrid procedures were conducted, consisting of three cochlear implantations, one intracochlear schwannoma resection followed by cochlear-implantation, four tympanoplasties (including two revision cases), two parotidectomies and one microvascular anastomosis of a radial free flap. The exoscope was used and evaluated by four experienced head and neck surgeons with assistance from two ENT-specialists, a resident and a final-year medical student. There were no complications during or after the surgery. Figure 2 shows the operation room setup, for cochlea implant (CI) surgery (a), for the microvascular anastomosis (b) and for the parotidectomy (c).
Fig. 2
Operation room setup with placement of the KINEVO® 900 S from ZEISS. The ZEISS KINEVO 900S is seen in sterile draping, the oculars and the hand bars are still attached. The ZEISS KINEVO 900S is placed in adequate distance from the surgical field, without interfering with the surgeons’ movements or the surgical field. The figure shows exemplarily a a cochlear implant surgery, the surgeon on the left side is currently conduction mastoidectomy, both the surgeon and the assistant wear 3D-glasse, b the conduction of a microvascular anastomosis with the usage of the 3-D glasses for both surgeon and assistant currently conducting the venous anastomosis of a radial free flap and c a parotidectomy with the assisting surgeon using the Head-mounted display (HMDmd). The system is currently limited to the two presented monitors, the assisting surgeon is not looking at a third monitor, the visualization of the surgical field is possible with the HMDmd only
Nine out of these eleven cases were conducted entirely exoscopic. In one case, the second parotidectomy, we decided to start the surgery with the preparation of the skin flap and visualization of the parotid capsule without magnification, as we noticed a time and comfort disadvantage when starting exoscopic in the first parotid surgery (20 min vs. 30 min). In one of the three standard cochlear implant surgeries and during the resection of the intracochlear schwannoma, the surgeons opted to switch to the microscopic view for the insertion of the CI electrode and the wide cochleostomy respectively, as they felt more comfortable with the familiar technique and were still adapting to the new approach. The switch between exoscope and microscope was easy and seamless, thanks to the ZEISS KINEVO 900 S’s hybrid capabilities, which allow it to function as both an exoscope and a microscope.
An overview of the procedure types, number of cases, and surgical approach is provided in Table 1.
Table 1 Overview of procedures, number of cases, and surgical approachNo facial nerve injuries, wound healing disturbances, or exoscope-associated complications were observed. One instance of transient dizziness occurred after cochlear implantation, and one tympanoplasty required intraoperative prosthesis exchange due to anatomical complexity. In all other cases, postoperative outcomes were uneventful and consistent with the expected clinical course.
Time measurementThe startup time for the ZEISS KINEVO 900 S was on average 1:38 min, which is highly efficient given the system’s complexity. The time required for sterile draping of the exoscope was 2:04 min (range 1:50–2:30 min), which is approximately the same as the time needed for draping a conventional microscope. The total setup process, including draping and positioning the microscope over the surgical site, took an average of 4:14 min (range 4:05–4:45 min).
Mean time for cochlea implant surgery (incision-to-suture time) with the exoscope was 104 min. Depending on anatomic conditions cochlea implant surgery takes regularly between 80 and 150 min with a conventional microscope. Mean time for tympanoplasty was 102 min (conventional microscope 60–150 min), for the parotidectomy 135 min (conventional microscope: 60–180 min) and for microvascular suturing of the artery 19 min and of the vein 25 min (conventional microscope: ca. 20–30 min each for artery/vein).
Ergonomic assessmentErgonomic assessment was conducted in all eleven procedures for the primary surgeon and the assisting surgeon separately using the RULA method demonstrated superior ergonomics for all procedures performed compared to conventional techniques. This benefits both the primary surgeon and the assistant, as seen in Table 2.
Table 2 Average ergonomic stress according to the Rapid Upper Limb Assessment (RULA), a screening tool designed to quickly assess ergonomic risk factors that may contribute to musculoskeletal disorders (MSDs) of the upper limbsIn cochlea implant surgery and tympanoplasty, the standard use of a microscope caused significant strain on the head and neck. One surgeon exhibited hyperextension of the neck and back to achieve the desired viewing angle, while another experienced up to a 20-degree neck flexion when using the microscope’s ocular. Forward bending of the upper body and neck was also observed during parotidectomy and microvascular anastomosis, especially for the assistant surgeon. These issues were largely addressed by the exoscopic approach, as it allowed for a straight posture of the head and back, regardless of the desired field of view.
In terms of ergonomic strain on arms and hands, all surgical procedures showed moderate upper limb strain. However, this could only be partially improved through the exoscopic approach.
Visualization/evaluation questionnaireFigure 3a summarizes the surgeons’ evaluation concerning the comparison of the ZEISS KINEVO 900 S with other standard magnification devices (binocular microscopes and surgical loupes). Figure 3b shows the surgeons’ assessment of the pros and cons of the ZEISS KINEVO 900 S concerning comfort and feasibility.
Fig. 3
Surgeons’ evaluation (n = 8) of the KINEVO® 900 S according to a custom evaluation questionnaire handed to each surgeon after surgery. a Summary of the surgeons’ evaluation concerning the comparison of the ZEISS KINEVO 900 S with other standard magnification devices (binocular microscope and surgical loupes). The surgeons rated on a 5-point Likert-scale which device was favored depending on the conducted surgery depending on different rating categories like the depth of the surgical field or illumination. The assessment was conducted for each type of surgery separately, in case of different answers from the surgeons a median value was formed. M = microvascular anastomosis, P = parotidectomy, E = ear surgery. 1 = microscope/surgical loupes clearly favored, 2 = microscope/surgical loupes slightly better, 3 = neutral, 4 = exoscope slightly better, 5 = exoscope clearly favored, b Assessment of the pros and cons of the ZEISS KINEVO 900 S concerning comfort and feasibility rated on a 5-point Likert-scale. In case of different answers from the surgeons a median value was formed. 1 = very poor/strongly disagree, 2 = poor/disagree, 3 = neutral, 4 = good/agree, 5 = very good/strongly agree
The surgeries were performed without any problems or technical failures. A comfortable surgical working distance was maintained and there was no visual reduction of the surgical field due to the positioning of the exoscope. There were no significant modifications to the surgical techniques, and the operating room space was easily managed since the ZEISS KINEVO 900 S is similar in size to a traditional microscope.
Only in case of the parotidectomy the surgical loupes were seen as equivalent to the exoscope as magnification device. This was because one the one hand, handling an analog magnification tool, such as surgical loupes, requires significantly less effort compared to operating the technically sophisticated exoscope. On the other hand the magnification of the surgical field was described as better with the exoscope. Additionally, from the assistant’s point of view, the use of the exoscope as a teaching tool, justifies the effort required for preoperative setup and intraoperative handling.
Additionally, while surgical loupes only need to be put on, the exoscope requires powering up, connecting, and draping, which can be time-consuming. This gave surgical loupes an advantage in terms of preoperative ease of handling technical equipment. When comparing otologic and microvascular surgeries, there was no preference in the preoperative setup as the ZEISS KINEVO 900 S required similar preparation as a standard operating microscope.
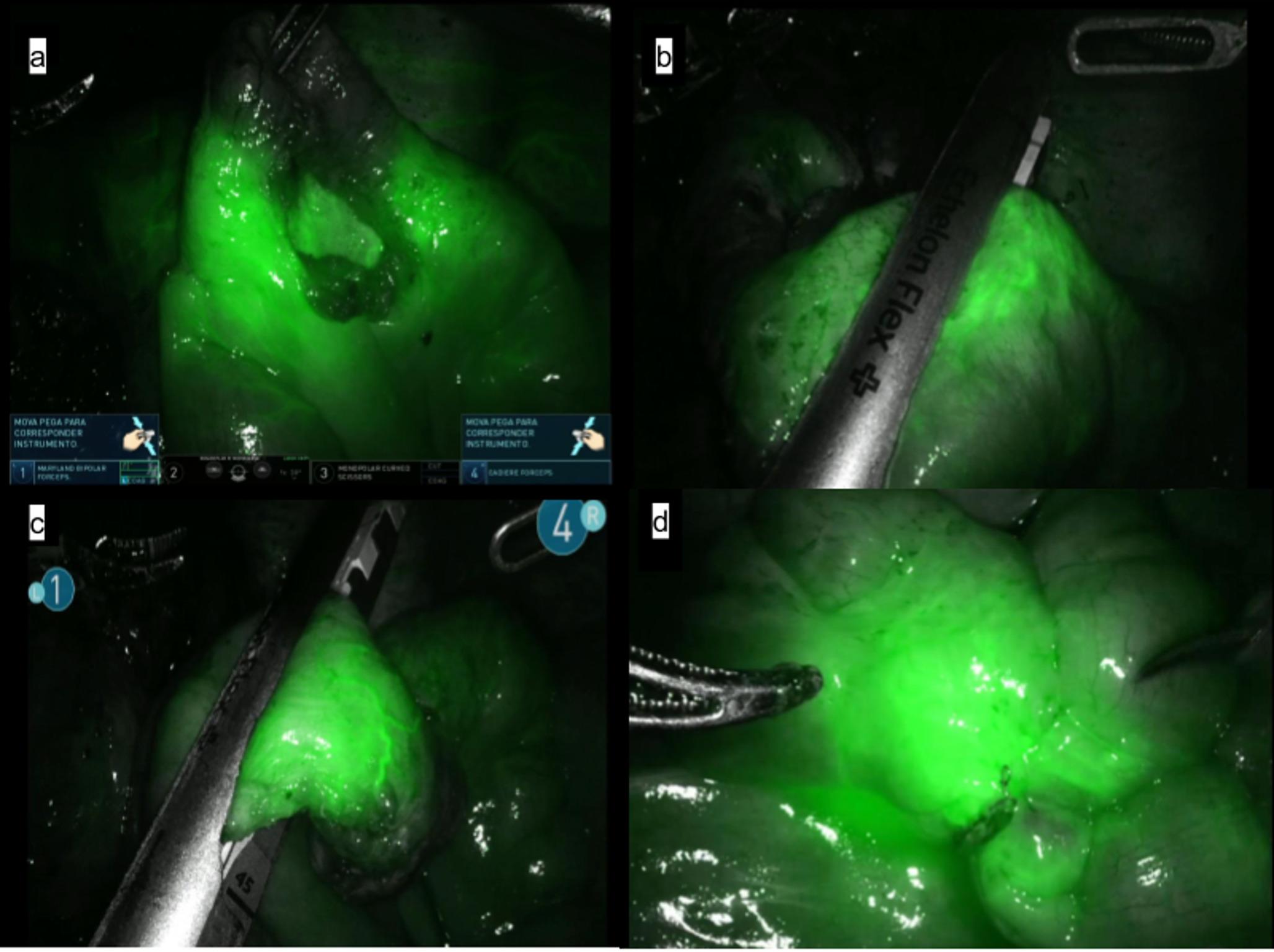
The 4 K-3D resolution provided an exceptionally sharp and detailed visualization of the surgical field. The polarized glasses required for 3D viewing were comfortable to wear. They did not obstruct the view of the instruments or the surgical site when the head was turned away from the monitor. There have been no reported cases of headaches or fatigue during surgery due to wearing the 3D glasses. Overall, there was no noticeable difference in image quality between viewing the surgical field on the monitor with 3D glasses and through the oculars of the microscope. In middle ear surgery the depth of the surgical field and the identification of anatomical structures have even been described as being more favorable for the exoscope than the microscope. Figure 4 shows the intraoperative exoscopic image in a case of cochlear implant surgery (a + b) and in a case of tympanoplasty (c + d). During parotidectomy the illumination of the surgical field and its magnification were found to be better than with the use of surgical loupes. Figure 5 illustrates the intraoperative image during parotidectomy (a) with visualization of the facial nerve as well as the conduction of a venous and aterial anastomosis in the conduction of a radialis free flap (b).
Fig. 4
Intraoperative exoscopic image of the ZEISS KINEVO 900S in a case of cochlea implant surgery after mastoidectomy, antrostomy and cochleostomy (a) and insertion of the cochlear electrode into the round window (b), in tympanoplasty after mastoidectomy and antrostomy with visualization of the stapes suprastructure and the long process of the incus (c) and after placement of an angular clip protheses connecting the long process of the incus with the stapes suprastructure (d).  round window visible after mastoidectomy,
round window visible after mastoidectomy,  Cochlea Implant electrode inserted into the round window,
Cochlea Implant electrode inserted into the round window,  chorda tympani,
chorda tympani,  stapes superstructure,
stapes superstructure,  long process of the incus,
long process of the incus,  angular clip prothesis connecting the long process of the incus and the stapes superstructure
angular clip prothesis connecting the long process of the incus and the stapes superstructure

Intraoperative exoscopic image of the ZEISS KINEVO 900S during laterocaudal parotidectomy a with visualization of the facial nerve, the tumor mass is resected with the lateral part of the parotid gland, b resection of a parotid tumor mass. Intraoperative exocopic image during microvascular anastomosis of a radial free flap for reconstruction of an oropharyngeal defect after tumor resection (c + d) with arterial anastomosis of the radial artery and the superior thyroid artery (c) and venous anastomosis of the internal jugular vein and the median cubital vein (d).  Facial nerve,
Facial nerve,  tumor,
tumor,  healthy parotid tissue,
healthy parotid tissue,  Radial artery,
Radial artery,  superior thyroid artery,
superior thyroid artery,  internal jugular vein,
internal jugular vein,  median cubital vein
median cubital vein
All surgeons highlighted the educational benefits of the exoscopic view. Additional oculars mounted on conventional microscopes are often difficult to reach for the assisting surgeon or student. In addition, the orientation and the field of view through the assistant’s ocular is often slightly different from the surgeon’s view. Traditional microscope monitors have historically displayed a 2D image with less detail and brightness than the original image through the ocular. This was a disadvantage especially in middle and inner ear surgery, where orientation in a 2D image is difficult in the narrow and deep spaces of the middle and inner ear.
When testing the HMDmd, one of the assisting surgeons complained of headaches after approximately one hour of surgery due to the pressure and weight of the device. However, the visualization of the head-mounted display was described as accurate and well detailed. An advantage was that the surroundings in the operating room could be seen while wearing the head-mounted display. This is important for patient safety, especially during parotidectomy when facial nerve stimulation must be visually recognized.
Robotic control and AI-assisted functionalitiesOne of the most significant adjustments for the surgeon involved adapting to microscope positioning via foot pedal rather than the conventional handgrip controls. While this required an initial adaptation period, it ultimately facilitated continuous bimanual operation and improved surgical efficiency. The foot pedal can be individually programmed for each surgeon, allowing for customization of robotic motion speed and control settings of the Cobotic Assistant Functionality.
The integration of Voice Control was particularly appreciated by the surgeons as it allowed hands-free operation of key functions, such as photo and video documentation, light intensity adjustment, position memory activation, and setting of different movement modes. This feature reduced the workload for the operating room staff and facilitated the control of the exoscope for the surgeon.
The Point-Lock function was particularly useful during otologic procedures such as tympanoplasty, allowing efficient inspection of the tympanic cavity from various angles without the need for repositioning. The ability to maneuver the microscope around a fixed focal point was also advantageous during parotid surgery and microvascular anastomoses.
The Z-mode facilitated smooth exoscopic operation but revealed its limitations when the system’s maximum working distance of 625 mm was reached. Autofocus performance was occasionally suboptimal at this range, requiring manual adjustments via foot pedal. In a smaller distance (up to 550 mm) the autofocus worked reliably.
Comments (0)