Robotic liver resection (RLR) is gaining fast worldwide implementation as minimally invasive liver surgery over the laparoscopic approach, although being considered a “non-inferior approach” and a “development in progress” technique [1]. Notwithstanding, despite the lack of high-quality evidence, the implementation of robotic platform advantages push experienced surgeons to perform increasingly complex and demanding hepatic procedures [2].
Nonetheless, liver parenchymal transection (LPT) is still one of the most technically demanding and challenging steps during advanced RLR. The lack of external nor internal anatomical landmarks, homogeneous methodology, and the heterogeneous use of different transection tools [3], leads to an important bias that makes it difficult to compare clinical outcomes between different surgical centers [4], but also to achieve a consensus in its standardization.
According to the available literature, RLR can be classified as hybrid or robotic-assisted, totally or fully robotic, and real or pure robotic.
On one hand, hybrid or robotic-assisted is considered “two-surgeon technique”, because the scrubbed assistant surgeon plays a leading role with laparoscopic tools through the accessory assistant trocar, usually the CUSA dissector. This method may be limited due to its zero degrees of wrist movement, representing a challenging step for the scrubbed surgeon, because of the arch restrictions from the accessory trocar, but leaving apart the full potential of dissection of the robotic arms.
On the other hand, totally or fully robotic approaches are considered “one surgeon techniques”, because the leading surgeon performs the whole procedure from the console, with no use of external laparoscopic tools. The limitation in that case is not to count on the advanced laparoscopic tools, nor the CUSA.
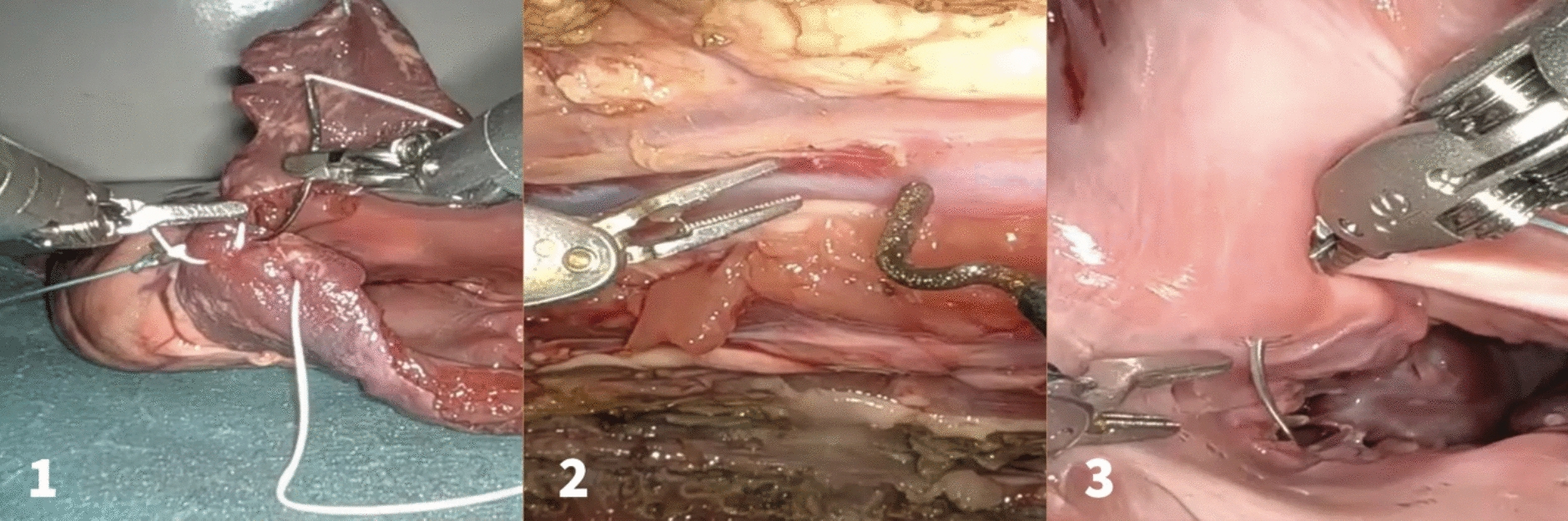
While the totally or fully robotic approach includes the use of the full catalog of advanced energy instruments, just as the Synchroseal®, the real robotic (RR) or pure robotic approach, is also a “one surgeon technique”, but only counting on the platform’s standard default tools (mainly forceps and scissors), and the selective use of the bipolar and monopolar energy, respectively, what can be defined as the minimum common technical option available to perform the RR LPT [5]. This technical baseline represents a highly reliable option to set a standardization.
The WHO has defined standardization as the process of “developing, agreeing upon and implementing uniform technical specifications, criteria, methods, processes, designs or practices that can increase compatibility, interoperability, safety, repeatability and quality” [6]. This need goes through audit and mature reflection when introducing a new surgical technique [7]. As such, setting standards to improve quality and reach the next level of care is key to ensure a rollback of the wheel of continuous improvement [8], embracing the IDEAL framework [9].
Assuming that to set a standard RR LPT is the key milestone to improve the comparability of outcomes, as well as facilitate reliable comparisons between hepatobiliary centers worldwide, it is arguable to specify the methodology in terms of safety and reproducibility. This way, the easiest path to reproducibility is to state basal techniques, and to define its steps, to set the minimum common approach from which to implement technical improvements.


Comments (0)