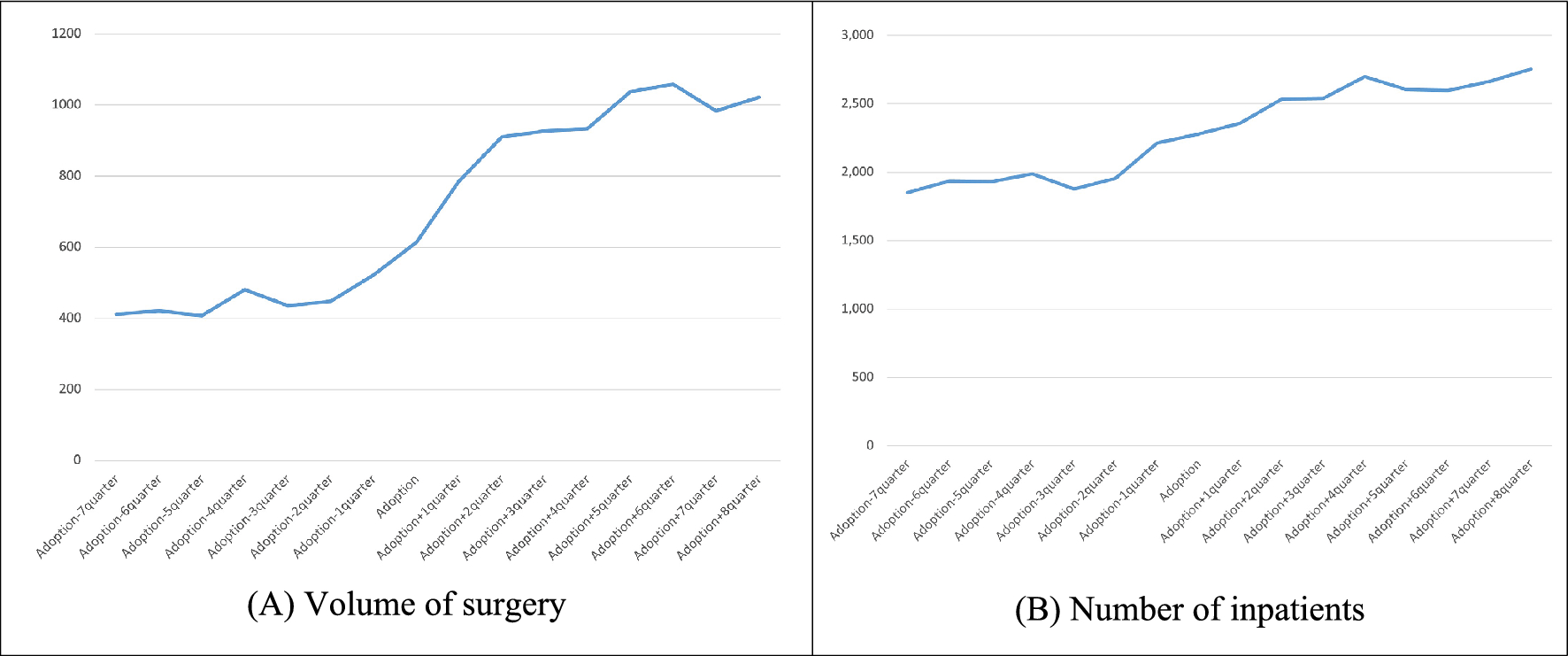
This study was conducted to investigate the impact of robotic surgery adoption on service volumes, focusing on prostate and thyroid cancers, which account for more than half of the robotic surgeries performed in South Korea. Analyzing the impact of robotic surgery at the institutional level showed that hospitals adopting robotic surgery experienced an increase in the volume of services for both prostate and thyroid cancers. For prostate cancer, the volume of surgeries increased by approximately 4.9 cases per quarter immediately after the adoption of robotic surgery, with a more substantial increase in the volume of surgeries and inpatient admissions compared to the pre-adoption period. For thyroid cancer, the number of inpatient admissions showed a significant increasing trend after the adoption.
The increase in service volume at hospitals that adopted robotic surgery can be interpreted in several ways. Firstly, these hospitals may have already been strategically aiming to increase service volume. Secondly, they may have actively worked to achieve the expected service volume targets upon adopting robotic surgery, which might have contributed to supplier-induced demand. Additionally, the advertising effect of adopting robotic surgery might have attracted more patients from surrounding areas, increasing service volume [13, 16]. Institutions that adopted robotic surgery also showed an increasing trend in PSA test volumes compared to the pre-adoption period. This result suggests efforts by hospitals to increase the volume of services for prostate cancer patients after the adoption of robotic surgery.
These findings support previous studies that suggest the adoption of robotic surgery increases service volumes at medical institutions [16]. For instance, a study in Wisconsin, USA, found that after adopting robotic surgery, the number of prostatectomy patients increased by about 114% over three months compared to institutions that did not introduce robotic surgery. Other studies in the USA have also shown a significant increase in prostatectomy rates at hospitals that adopted robotic surgery compared to those that did not [14]. This increase in service volume at institutions adopting robotic surgery may have led to the concentration of patients. Institutions that adopt robotic surgery may attract patients from nearby facilities that have not adopted the technology, leading to a concentration of surgical demand at the adopting institutions. Previous studies have also shown that in regions where robotic surgery is adopted, demand tends to concentrate at the institutions that adopt it [17,18,19,20].
The significance of this study lies in several areas. Firstly, this study provides evidence of the causal relationship between the adoption of robotic surgery and the subsequent increase in service volume at the institutional level. The increase in service volume, driven in part by the concentration of patient demand at institutions with robotic surgery capabilities, suggests that the adoption of high-cost medical technologies can lead to shifts in healthcare delivery patterns, potentially increasing overall healthcare expenditures. Secondly, the study serves as a critical foundation for further research on the impact of expensive medical technologies in healthcare systems. By examining the robotic surgeries adoption in South Korea, the study sheds light on how such technologies are integrated into clinical practice and how they may influence institutional strategies and patient behavior.
This study has several limitations. Firstly, it did not cover all diseases treated with robotic surgery—such as colorectal cancer or uterine myoma—but focused on prostate and thyroid cancer. As robotic surgery continues to expand across specialties, future research should include a broader range of diseases. Secondly, although we observed an increase in the volume of medical services following the adoption of robotic surgery, it remains unclear whether this was driven by supplier-induced demand, strategic institutional behavior, or the advertising effects of robotic surgery adoption. These are speculative interpretations, as they were not empirically tested in the present study. Third, the generalizability of our findings may be limited and should be interpreted with caution, particularly beyond the context of South Korea. Although South Korea operates a single-payer system for most healthcare services, robotic surgery is a non-reimbursed service typically paid out of pocket or through supplementary private health insurance. Therefore, provider and patient behaviors surrounding robotic surgery in South Korea may resemble those seen in multi-payer contexts. This nuance should be considered when applying our findings to other healthcare contexts. Future research comparing the adoption and impact of robotic surgery across different healthcare systems would help clarify the role of institutional context in shaping these outcomes.
The analytic approach used in this study warrants careful consideration. Although this study employed ITSA to strengthen causal inference, it faces limitations related to both the assumptions required for ITSA and the absence of an external control group. ITSA assumes that no concurrent institutional or policy changes occurred and that the pre-adoption trends were linear—assumptions that may not always hold in complex healthcare settings. Given the staggered timing of robotic surgery adoption across hospitals, we could not verify the absence of policy changes at each adoption point. However, in South Korea’s single-payer healthcare system, national policy changes, when implemented, are typically applied uniformly across institutions, and the temporal dispersion of adoption reduces the likelihood that a single policy change systematically biased the results. Additionally, visual inspection of pre-adoption trends supported the plausibility of linearity in this context. While ITSA allows each institution to serve as its own control by comparing pre- and post-adoption trends, the lack of a non-adopting comparison group limits our ability to rule out broader secular trends or contemporaneous system-level shifts. To strengthen causal interpretations, future research could identify counterfactual control groups and/or incorporate multiple-group ITSA. Comparative designs such as matched control groups and difference-in-differences analysis may also improve the strength of causal argument.
In conclusion, the findings of this study underscore the substantial impact of robotic surgery adoption on medical service volumes and its broader implications for healthcare costs and institutional strategies.


Comments (0)