This study evaluated the CT findings of bear-inflicted injuries using the FISS, Marshall Head-CT Classification, AAST chest wall injury grade, and Superficial and Muscular Injuries of the Limbs and Trunk. The FISS score and AAST chest wall injury grade were significantly associated with hospitalization duration. Additionally, the inter-observer agreement for the FISS scores, Marshall Head CT Classification, AAST Chest Wall Injury Scale, and superficial and muscular injuries of the limbs and trunk was excellent, supporting the reliability of our imaging evaluations.
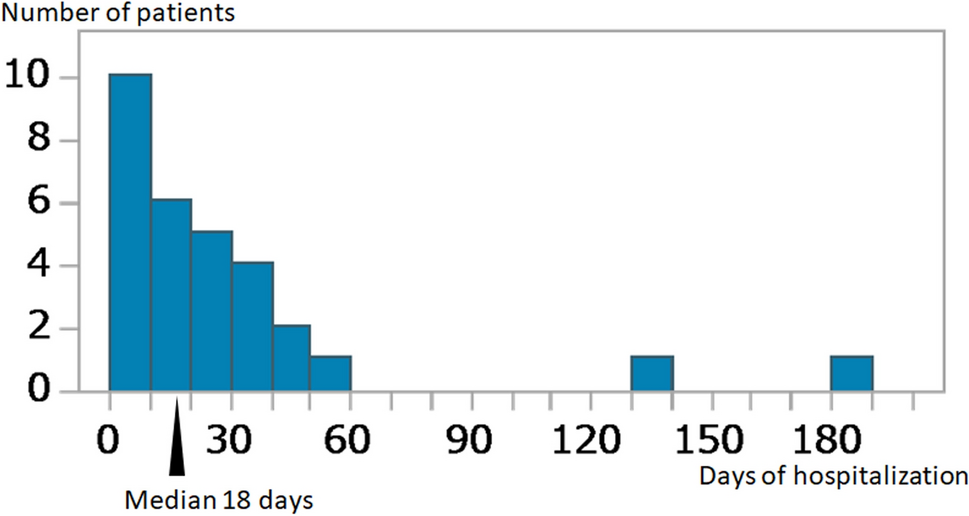
In our study, 71.0% of bear attack victims were male, and the median age was 72 years, indicating that the affected population was predominantly elderly. Previous reports have documented that bear attack victims are overwhelmingly male and almost exclusively adults, which is consistent with our findings [14, 15]. The mean hospitalization duration has been reported as 22 days [16], which is not markedly different from the median of 18 days in our study. Fatalities due to bear-inflicted injuries were observed in one case (3.2%) in our study. Bear attacks of the present study in Akita Prefecture, located in the northeast region of Japan, are believed to be caused by the Asiatic black bear [3, 17]. A previous study analyzing 417 cases of bear-inflicted injuries attributed to black bears reported a mortality rate of 2.4% [18], which is comparable to our findings. However, our mortality rate of 3.2% reflects only cases of bear-inflicted injuries among patients transported to the hospital. Cases of prehospital deaths, including those discovered as unexplained deaths and subsequently examined by forensic autopsy, were not included in our analysis, which may affect the accuracy of the mortality rate.
Our findings demonstrate that patients in the long hospitalization group had significantly higher FISS scores and higher AAST chest wall injury grades than those in the short hospitalization group in multivariate analysis. This result is consistent with previous studies on maxillofacial trauma, including those not limited to bear-inflicted injuries, where higher FISS scores have been associated with increased treatment complexity, longer recovery times, and the need for multidisciplinary care [9, 11]. In a previous study, FISS scores ranged from 1 to 12 [19]. In contrast, the FISS scores in our study, which focused on bear-inflicted injuries, showed a wider distribution, with a maximum score of 33. This finding suggests that bear- inflicted maxillofacial injury tends to be more severe than general maxillofacial injuries. Additionally, the Marshall Head-CT Classification (i.e., the presence or absence of Diffuse Injury II) did not differ significantly between the short and long hospitalization groups in univariate analysis. In our cohort, head injuries consisted of one case of cerebral contusion and four cases of subdural hematoma. These findings indicate that, in bear-inflicted injury cases, maxillofacial injury and chest injury might have a greater impact on hospitalization duration than head injuries.
The distribution of maxillofacial injuries in our study showed that midface scores were generally high. This finding aligns with previous reports indicating that maxillofacial fractures caused by bear attacks predominantly occur in the midface region [20]. Previous reports concerning laterality in bear-inflicted injuries include both unilateral and bilateral cases. Unilateral cases have been associated with severe maxillofacial injury and eye injuries, with one study reporting that 15% of cases had unilateral eye injuries, all resulting in vision loss [21]. In contrast, bilateral maxillofacial fractures have also been reported, although these findings are based on a limited number of cases, and no large-scale statistical study has conclusively demonstrated clear laterality differences in bear-inflicted injuries [22,23,24]. In our sub-analysis, we observed statistically significant bilateral correlations in midface and upper face injuries, with a corresponding correlation between midface and upper face scores. Conversely, mandibular fractures appeared to occur independently on each side, possibly reflecting asymmetric bite forces or unilateral defensive injuries sustained during an attack. Furthermore, no significant differences were found when comparing the FISS scores between the right and left sides. Based on these results, we demonstrated that in bear-related injuries, midface and upper face injuries often occur simultaneously and are frequently bilateral. The frequent bilateral injuries to the midface and upper face may be attributed to the fact that bears, as highly intelligent animals, tend to target the upper part of the face to weaken their opponent and prevent retaliation [25]. In a previous study of 469 patients with maxillofacial trauma, mandibular fractures were the most common injury type [11]. The study population mainly consisted of patients who had sustained injuries from traffic accidents and interpersonal violence. Both of these causes are typically associated with mandibular trauma. In contrast, our findings suggest that midface fractures are more characteristic of bear-inflicted injuries. A previous study reported that eye injuries occur in 59% of cases, and 23.5% of patients are permanently blind in one eye [8]. Although eye injuries are not included as an evaluation item in the FISS scoring system, they are believed to significantly impact post-injury aesthetics and quality of life (QOL). It has been reported that even after the acute phase and hospital discharge, patients with maxillofacial injury experience an increased incidence of Post-Traumatic Stress Disorder (PTSD), higher rates of alcohol dependence, and a decline in QOL [26]. Therefore, if outcomes such as appearance and QOL are to be assessed, a separate scoring system that includes eye injuries may be necessary.
Although no simplified version of the FISS has been established to date, we explored the potential utility of region-specific scores in the supplemental analysis. In Table 5, we compared the FISS sub scores between the short and long hospitalization groups. Notably, the Total Midface Score showed a statistically significant difference between the two groups, with a p-value comparable to that of the Total FISS Score. This finding suggests that the Midface Score alone may potentially serve as a simplified indicator of facial injury severity. However, due to the limited sample size in each group (n = 15), the generalizability of this finding remains uncertain. Further research with larger patient cohorts is warranted to validate this approach and to develop a simplified assessment method for clinical use.
In this study, the one mortality case was an 84-year-old man with a FISS score of 31 and a right subdural hematoma. Previous studies have not reported a direct association between FISS scores and mortality. Instead, factors such as age, Glasgow Coma Scale (GCS) scores, and the Injury Severity Score (ISS) have been identified as being associated with mortality in maxillofacial injury [27]. The ISS calculates trauma severity by summing the squares of the three most severe injuries, each scored from 1 (minor) to 6 (unsurvivable), based on the Abbreviated Injury Scale (AIS) [28]. The AIS is a standardized system that assigns severity scores to individual injuries across different body regions, providing the foundation for ISS calculations. Since there was only one fatality in this study, further investigation into factors related to mortality in bear-inflicted injuries would require multi-institutional studies or the inclusion of fatal cases from forensic analyses.
AIS is a widely used scoring system for assessing trauma severity. However, AIS evaluation, which incorporates multiple aspects such as clinical findings, surgical reports, and imaging data and relies on detailed coding, is time-consuming. In contrast, CT-based scoring systems, such as FISS, the Marshall Head-CT Classification, and the AAST Chest Wall Injury Scale, allow for an objective assessment of bear-inflicted injury severity based solely on radiological findings. The CT-based scoring in this study was a combination of existing scoring systems proposed for different anatomical regions. Although AIS was not used in this study, a key strength of our study is that FISS and the AAST Chest Wall Injury Scale, both derived from objectively obtained initial CT images, were found to be associated with hospitalization duration.
This study has several limitations. First, the sample size was small due to the rarity of bear-inflicted injuries. Larger, multi-institutional studies are needed to validate our findings. Second, this study was retrospective and compared initial CT findings from bear-inflicted injuries with hospitalization duration without evaluating treatment variability or post-discharge QOL. Future studies should investigate the relationship between initial CT findings, treatment variability, and post-discharge QOL to provide a more comprehensive understanding of outcomes in bear-inflicted injuries. Moreover, potential postoperative complications, such as infection or occlusal dysfunction, were not assessed in this study. These factors may directly influence not only long-term outcomes and patient QOL, but also hospitalization duration itself. Therefore, future studies should investigate the relationship between initial CT findings, postoperative complications, treatment variability, and post-discharge QOL to provide a more comprehensive understanding of outcomes in bear-inflicted injuries.
In conclusion, FISS score and AAST chest wall injury were significantly associated with hospitalization duration in bear-inflicted injury. In a detailed analysis of FISS scores, midface, and upper face injuries often occur simultaneously and bilaterally.


Comments (0)