
Remember me
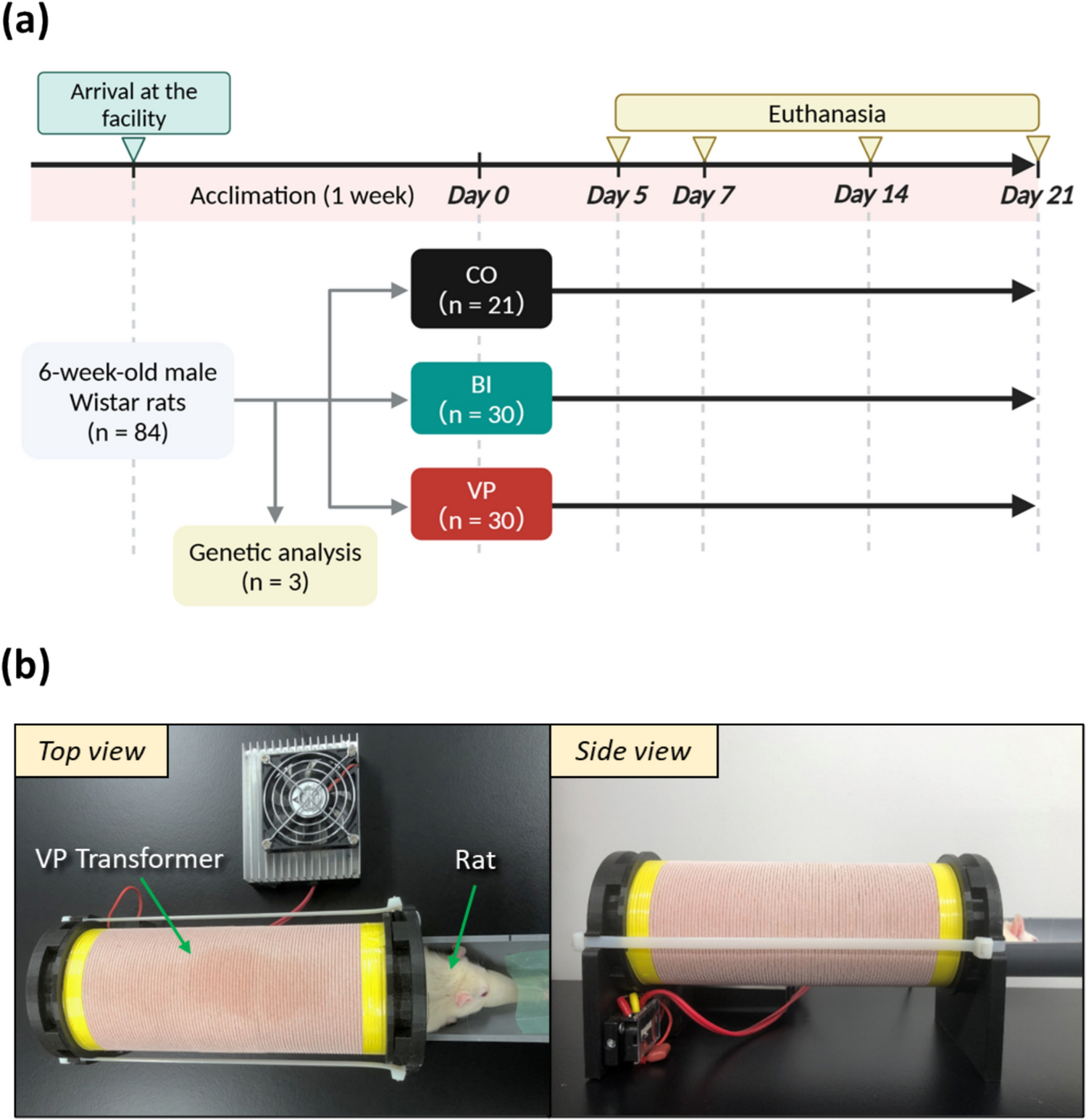
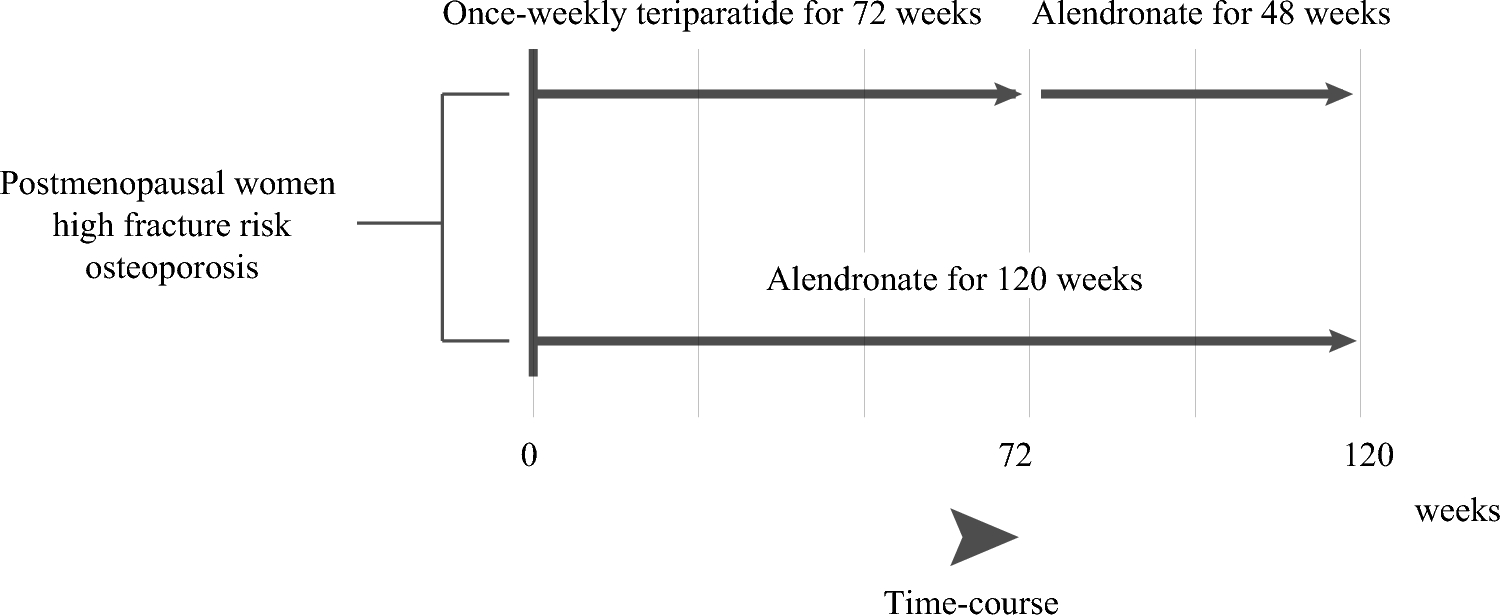
The JOINT-05 study was a prospective, randomized, open-label, blinded-endpoint trial conducted between October 2014 and June 2020 at 113 institutions in Japan. This study is a sub-analysis of the JOINT-05 trial, which was conducted as part of the Adequate Treatment of Osteoporosis (A-TOP) research group, and Japanese women aged ≥ 75 years were enrolled if they had primary osteoporosis and were at high risk of fracture. The detailed design, eligibility, and baseline characteristics of JOINT-05 have been described previously [14,15,16]. Participants were randomly allocated in a 1:1 ratio to two groups: sequential therapy with once-weekly TPTD for 72 weeks followed by once-weekly ALN for 48 weeks (TPTD group); or monotherapy with ALN for 120 weeks (ALN group). Both groups received daily supplements of 400 IU of native vitamin D throughout the entire treatment period. The design diagram is shown in Fig. 1. This study was conducted in accordance with the Declaration of Helsinki and was approved by the central and onsite institutional review boards. Informed consent was obtained from all participants.
Fig. 1
Drug administration periods and study flow by group
This study was a subgroup analysis of the primary and secondary fracture endpoints, specifically aimed at elucidating outcomes in patients with frailty [17]. Physical frailty was defined as a condition requiring support or nursing care, and cognitive frailty was defined as a Mini-Mental State Examination (MMSE) score of 27 or lower [18]. In the two groups randomly assigned in JOINT-5, patients with frailty were identified, and subgroup analyses were performed. In addition, the number of dropouts due to medication non-adherence was identified from the full analysis set. The dataset for these analyses comprised data finalized by the Joint Center for Researchers, Associates and Clinician (JCRAC) Data Center of the National Center for Global Health and Medicine on February 4, 2020, as well as the Week 120 fracture assessment results from the fracture assessment committee in October 2020, and the list of discontinued cases verified during a case review meeting in December 2022.
Baseline characteristics and outcomesThe baseline characteristics, laboratory measurements, QOL, and dietary intakes were collected at baseline. Baseline patient characteristics included age, age at menopause, years since menopause, body weight, height, and body mass index (BMI; calculated as weight in kilograms divided by height in meters squared). The number and grades of prevalent vertebral fractures, history of prior femoral fractures, osteoporosis treatment, and bisphosphonate use were also recorded. Bone mineral density (BMD, T-score) was measured at the lumbar spine, total hip, and femoral neck using dual-energy X-ray absorptiometry (DXA) at each participating institution. Comorbidities, including hypertension, diabetes mellitus, dyslipidemia, rheumatoid arthritis, osteoarthritis, and other conditions, as well as systolic and diastolic blood pressures, were documented. Cognitive function was evaluated using MMSE scores, categorized as ≥ 28, 24–27, and ≤ 23. Physical function was assessed with the timed up-and-go test and the one-leg standing test with eyes open. Social support levels were classified into five categories: support-required and nursing care levels 1, 2, 3, and 4–5. Laboratory measurements included bone turnover markers [osteocalcin (ng/mL), procollagen type I amino-terminal propeptide (P1NP; μg/L), and tartrate-resistant acid phosphatase-5b (TRACP-5b; mU/dL)], 25-hydroxyvitamin D (25OHVD; ng/mL), pentosidine (pmol/mL), HbA1c (%), total cholesterol (mg/dL), high-density lipoprotein (HDL) cholesterol (mg/dL), low-density lipoprotein (LDL) cholesterol (mg/dL), triglycerides (mg/dL), estimated glomerular filtration rate (eGFR; mL/min/1.73 m2), creatinine (mg/dL), albumin (g/dL), and calcium (mg/dL). Back pain severity was assessed using a visual analog scale (VAS), ranging from 0 to 100 points, and QOL was measured using the EQ-5D questionnaire. Nutrient intake was evaluated through a Food Frequency Questionnaire [19].
The study’s primary endpoint was morphometric vertebral fractures, and the secondary endpoints included clinical vertebral fractures, progression of vertebral fractures, non-vertebral fractures, and the overall incidence of all fractures at 0, 24, 48, 72, and 120 weeks. Adherence-related treatment discontinuation was defined based on pre-specified trial criteria, including voluntary withdrawal, prolonged interruption of TPTD therapy (> 8 weeks), complete discontinuation of ALN therapy, or other investigator-determined reasons. Discontinuation was determined using both physician judgment and patient self-reporting and was recorded at the last visit where these criteria were met. In the analyses of patient background characteristics related to adherence-related treatment discontinuation, compliance-related treatment discontinuation was defined as the primary outcome, and predictors were identified using univariable logistic regression analysis.
Statistical analysisNumerical and categorical data are described by means and standard deviation (SD) values and proportions, respectively. In the fracture analyses, multivariable Poisson regression models were used to estimate the rate ratios between the TPTD group and the ALN group, along with their 95% confidence intervals (CIs), using the generalized estimating equation (GEE) approach. The GEE-Poisson regression included age, counts, and maximum grades of prevalent vertebral fractures, history of proximal femoral fractures, and BMD at baseline as covariates and individual and institute as clusters. These variables were selected based on their specification in the original JOINT-05 study protocol and their established clinical relevance to fracture risk [14]. Superiority hypotheses for the incidences of morphometric vertebral fractures, any fractures, clinical vertebral fractures, and the progression of vertebral fractures and the non-inferiority hypothesis for non-vertebral fractures, defined as the upper limit of the 95% CI for the rate ratio being less than 1.96, were tested [15]. In the analysis of the contributions of patient background characteristics to adherence-related discontinuation, logistic regression models were used to calculate odds ratios (ORs) and 95% CIs. Potential predictors of adherence-related discontinuation were initially screened by univariable regression with P value < 0.05, followed by fitting with multivariable regression. Missing covariates were handled by multiple imputation, applying a monotone model specification. Multiplicity adjustment was not performed, because this was an explanatory analysis, and p values < 0.05 were considered significant. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC).
Comments (0)