
Remember me
This retrospective cohort study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Tohoku University (approval No. 2024–1-1026).
Data sourceThe data were retrospectively collected from Japan's nationwide administrative DPC reimbursement system database [26]. Comprehensive informed consent was obtained from all patients upon admission, covering both their agreement to the proposed treatment methods and permission for the academic use of data collected during their care. No personally identifiable information is included in this study. All variables used in the analysis were derived from this data source. Cases with missing values for any relevant clinical variables were excluded to ensure data completeness and accuracy. No imputation methods were applied, and only cases with complete data were included in the final analysis.
Inclusion and exclusion criteriaThe sample size for this study was determined based on a fixed study period rather than a priori power calculation. Patients were identified from a nationwide survey of hospitals participating in the Japanese DPC system, covering the period from April 2016 to March 2022. Approximately 1,100 DPC-participating hospitals consistently submitted medical records and were approved for inclusion in this study. The analysis included patients who underwent surgical treatment for hip fractures at these hospitals across Japan. This clinical investigation focused on elderly patients aged 65 years and older, specifically examining the incidence of postoperative complications and short-term in-hospital mortality among those with type 2 diabetes. Patients under 65 years of age and those treated conservatively for hip fractures were excluded. All eligible cases meeting the inclusion criteria during the study period were included to ensure a comprehensive representation of the target population.
Exposure of interestThis study examined patients who underwent surgical treatment for hip fractures, with a focus on comparing the incidence of postoperative complications during hospitalization between those with and without type 2 diabetes. Patients with type 2 diabetes were identified based on diagnostic codes (ICD-10 codes E11, E14, R730). Information on the duration and treatment of type 2 diabetes was not included in the analysis.
Outcomes of interestThe primary outcomes of this study were the incidence of postoperative complications and in-hospital mortality. These outcomes were selected due to their clinical relevance in evaluating the short-term risks associated with hip fracture surgery in elderly patients. The secondary outcomes were length of hospital stay and transfusion volume, which reflect healthcare utilization and perioperative management burden. The postoperative complications assessed in this study included venous thromboembolism, cardiac infarction, urinary tract infection, cognitive dysfunction, pneumonia, and in-hospital mortality. Postoperative cognitive dysfunction was identified using ICD-10 codes F010, F011, F012, F019, F03, F107, G238, G300, G301, G308, G309, G310, and G318, which encompass various forms of cognitive impairment and delirium occurring during the postoperative period, as previously described [19]. All outcomes were identified based on diagnostic codes. As mortality was included as one of the outcomes, the assessment period for all complications covered the entire duration of hospitalization. Secondary outcomes included length of hospital stay, total volume of perioperative blood transfusion, and the use of anti-osteoporotic medications.
CovariatesCovariates included age, sex, body mass index (BMI), type of anesthesia, fracture classification, surgical procedure, timing of surgery (categorized as within 2 days of admission or on/after day 3), comorbidities, including hypertension, ischemic heart disease, cerebrovascular disease, chronic renal disease, chronic lung disease, cognitive impairment. In addition, the Charlson Comorbidity Index, calculated from ICD-10 codes based on the original algorithm by Charlson et al. (1987) [27], was used to provide an overall assessment of comorbidity burden but was not included in the propensity score model to avoid redundancy with individual comorbid conditions. Age was included as a separate covariate in the analysis. Hip fractures were classified according to ICD-10 codes as follows: S7200 for femoral neck fractures, S7210 for trochanteric fractures, and S7220 for subtrochanteric fractures. Patients were selected for inclusion in the hip fracture cohort based on registry data, with eligibility determined by meeting all three of the following criteria: (1) principal diagnosis, (2) primary reason for hospital admission, and (3) condition associated with the highest medical resource utilization.
Propensity score matchingTo reduce confounding in the comparison of postoperative complications between patients with and without type 2 diabetes, a 1:1 propensity score matching was conducted based on clinically relevant covariates. The matching model included age, sex, BMI, timing of surgery, type of anesthesia, hip fracture classification, surgical procedure, and various comorbidities, including hypertension, ischemic heart disease, cerebrovascular disease, chronic renal disease, chronic lung disease, cognitive impairment, and the Charlson Comorbidity Index. Propensity scores were estimated using logistic regression, and nearest-neighbor matching without replacement was applied using a caliper width of 0.2 times the standard deviation of the propensity score estimates. Covariate balance after matching was evaluated using standardized mean differences (SMDs), with an SMD of less than 0.1 considered indicative of adequate balance. Multivariate logistic regression analyses were performed within the matched cohort to identify independent associations with outcomes, incorporating the covariates used in the propensity score model. The model's discriminatory performance was assessed using the C-statistic. This approach ensured a balanced comparison between type 2 diabetes and non-diabetes patients by minimizing baseline differences through adjustment for key confounders.
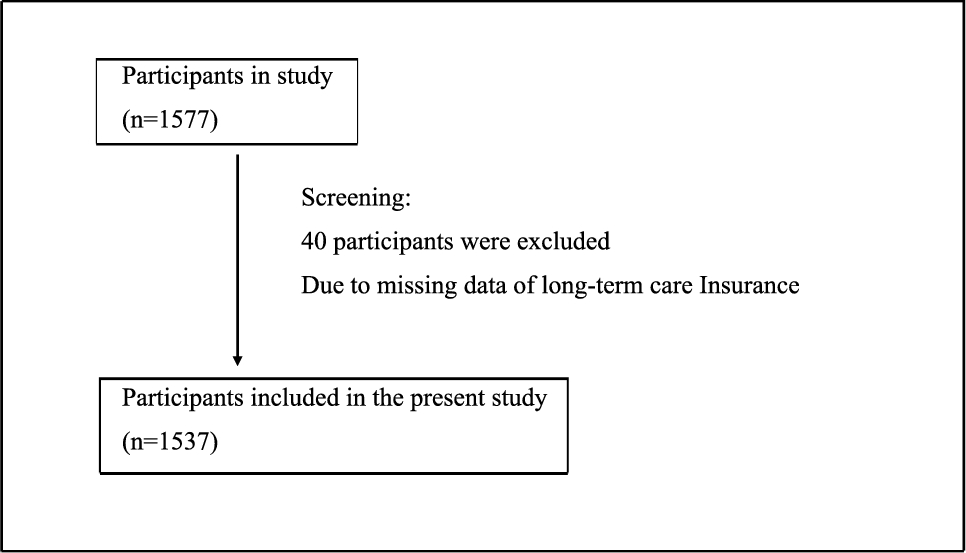
Figure 1 illustrates a schematic overview of the patient selection process. From the dataset covering the period between April 2016 and March 2022, a total of 474,293 patients met the predefined inclusion and exclusion criteria. Of these, 386,426 were classified as non-diabetes patients and 87,867 as type 2 diabetes patients. It was demonstrated that 18.5% of hip fracture cases among elderly individuals aged 65 years and older were associated with type 2 diabetes. Following 1:1 propensity score matching based on age, sex, BMI, various comorbidities, Charlson Comorbidity Index, timing of surgery, use of general anesthesia, type of hip fracture, and surgical procedure, matched cohorts were established, each comprising 83,283 patients in the type 2 diabetes and non-diabetes groups.
Fig. 1
Flow diagram of patient selection for type 2 diabetes and non-diabetes patients with hip fracture and propensity score (PS) matching. This diagram shows the method for extracting target patients from the DPC database and PS matching for type 2 diabetes and non-diabetes patients with hip fractures
Table 1 presents the baseline characteristics of patients with and without type 2 diabetes who underwent surgical treatment for hip fractures. Prior to propensity score matching, SMDs for sex, age, BMI, hypertension, ischemic heart disease, and timing of surgery exceeded 0.1, indicating notable imbalances between the groups. The type 2 diabetes group had a higher proportion of male patients, was generally younger, and exhibited higher BMI values. Furthermore, the type 2 diabetes group exhibited a higher prevalence of hypertension and ischemic heart disease, as well as a lower proportion of patients undergoing early surgery within 2 days of admission. Additionally, general anesthesia was more commonly used, and femoral neck fractures were the most prevalent fracture type among type 2 diabetes patients. Following 1:1 propensity score matching, all covariates—age, sex, BMI, comorbidities, Charlson Comorbidity Index, timing of surgery, use of general anesthesia, fracture type, and surgical procedure—achieved SMDs below 0.1, confirming adequate balance between the groups. The C-statistic for the propensity score model was 0.781, indicating good discriminatory ability.
Table 1 Characteristics of patients before and after propensity score matchingStatistical analysesData are expressed as mean ± standard deviation. Comparisons between the type 2 diabetes and non-diabetes groups were conducted using the χ2 test for categorical variables and Student's t-test for continuous variables. Univariate logistic regression analysis was performed to evaluate severe in-hospital complications and in-hospital mortality. Although SMDs indicated adequate balance between the groups after propensity score matching, a sensitivity analysis was conducted to account for the potential influence of unmeasured confounders. In this analysis, the caliper width for propensity score matching was tightened from 0.2 to 0.05, and similar risks of postoperative complications and in-hospital mortality were observed under these more stringent matching conditions, suggesting the robustness of our findings. To further confirm the consistency of the results, subgroup analyses were performed within the matched cohort by stratifying patients according to fracture type, specifically femoral neck fractures and trochanteric fractures. Survival differences between groups were assessed using the log-rank test. In consideration of the large sample size, a stringent significance level was adopted. All statistical tests were two-tailed, and a p-value of less than 0.001 was considered statistically significant. Statistical analyses were performed using JMP version 17 (SAS Institute Inc., Cary, NC, USA).
Comments (0)