Because of the deep anatomical structure and the hidden incidence, 80% of patients with HCC are diagnosed at an advanced stage with portal vein invasion, multiple lesions or multiple organ metastasis, and the prognosis is extremely poor (only 3–6 months without treatment) [22]. A study based on 342 patients by Uchino K [23] showed that the median OS rate was 8.0 months (range: 0.03–108.7 months) in patients with extrahepatic metastases of HCC. The lung is the most common metastatic organ of primary HCC, accounting for 39.5-53.8% of extrahepatic metastases in a previous clinical study [24]. Understanding the mechanism of lung metastasis of HCC will aid in the selection of individualized treatment plans. Currently, the known pathogenesis is presented as follows [25,26,27,28,29]: (1) HCC easily invades the hepatic or portal vein, forming hepatic artery-vein or portal-hepatic vein shunts, such that HCC cells can flow back into the pulmonary circulation through the hepatic vein; (2) the pulmonary circulation is a low-pressure system, with slow blood flow and easy stagnation of cancer cells; (3) the coagulation fibrinolysis activity of lung blood is higher, which is beneficial to the colonization and proliferation of HCC cells; (4) the abnormal expression of genes, proteins or exosomes plays a role in promoting the metastasis and invasion of HCC; and (5) TACE is clinically the most commonly used therapy for HCC at the BCLC A-C Stage, which is associated with the phenomenon of incomplete tumor-feeding arterial embolism, and the residual tumor will stimulate the high expression of vascular endothelial growth factor due to ischemia and hypoxia, thus upregulating the tumor’s invasion and metastasis ability. During clinical practice, because of the shorter OS and higher tumor burden of primary HCC, more clinical studies emphasize the importance of primary site treatment. However, there is no consensus strategy for cases where patients experience lung metastasis at initial diagnosis or after radical treatments such as LT, surgery, ablation, or TACE. Most clinicians believe that HCC enters a state of late systemic blood dissemination, and systemic chemotherapy or targeted therapy are frequently selected, although the benefit (PFS: 1.4–4.2 months) is still low based on a recent meta-analysis [30].
The state of malignant oligometastases refers to the intermediate state between the limited number and spatial distribution of metastatic lesions and progressive lesions (also known as multiple metastases) [31]. Because the biological behavior of tumors is relatively “mild”, local treatments can be more actively selected on the basis of systematic treatments. In the past 30 years, the status of oligometastases or oligoprogression has been confirmed in colorectal cancer, lung cancer, prostate cancer, and other solid tumors [32,33,34]. Taking liver and lung metastasis of colorectal cancer as an example, local treatments (e.g., surgery, SBRT, and ablation) are not only a model for multidisciplinary comprehensive treatment that is widely accepted by clinicians but have also been included in many international clinical guidelines [35, 36]. Compared with colorectal cancer, HCC is more invasive and has a shorter natural course. Thus, is local ablation for POs meaningful? Even in the latest international guidelines for the diagnosis and treatment of advanced HCC, there is no conceptual definition, diagnostic criteria, differential methods, or treatment specifications.
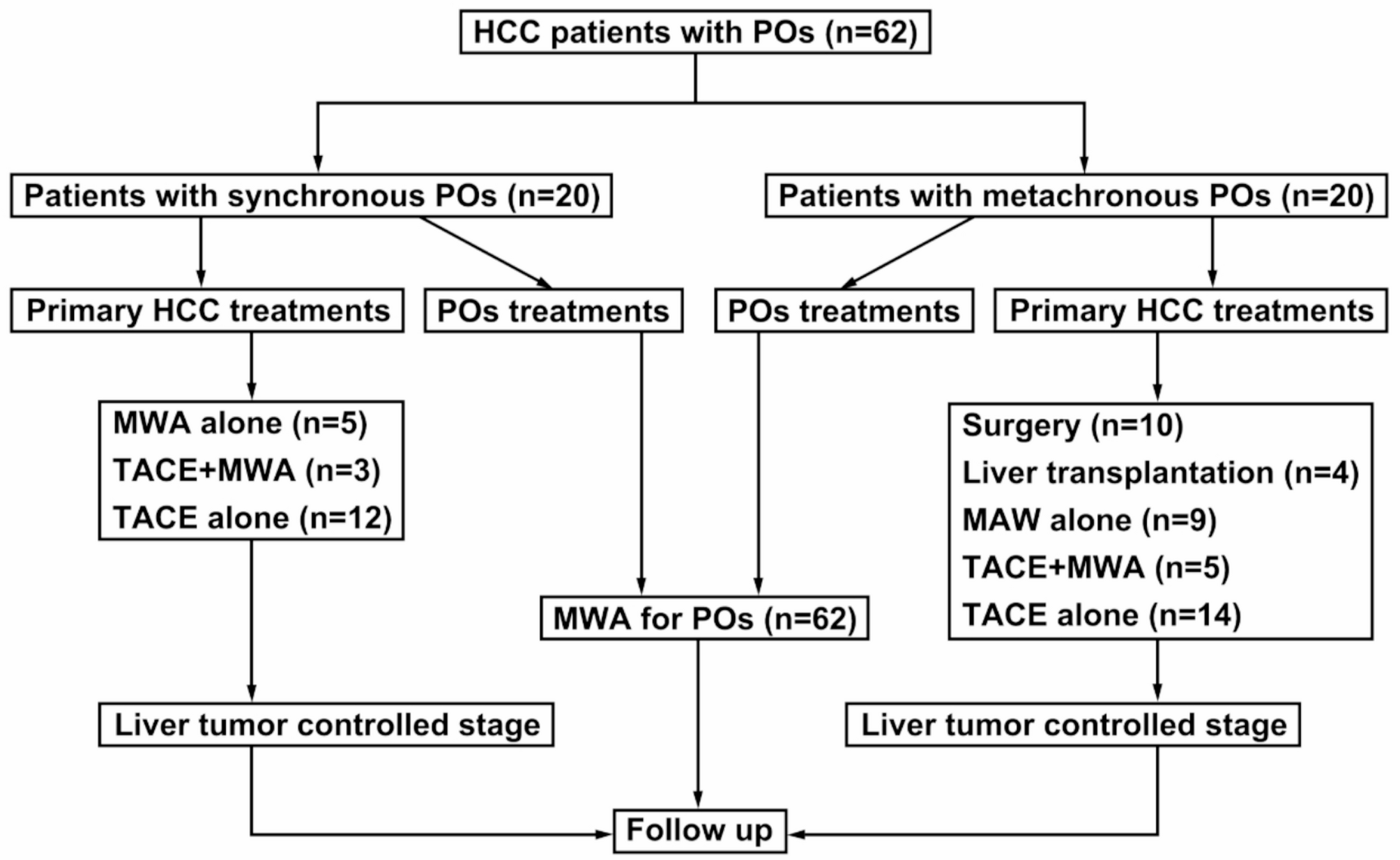
The present study described the outcome of POs from HCC treated with ablation. The technical success, technical efficacy, and major complication rates were 100%, 96.8%, and 21%, respectively, which were in accordance with the rates in previously published studies (91.0-100%, 61.5–100% and 0-34.3%, respectively) [37]. Compared with a median OS of 8.0 months in Uchino K’s [23] large-sample observational study on extrahepatic metastases from HCC, the median PFS and OS rates of 11.4 and 33.0 months in our study were better. Notably, 9.7% (6/62) of patients survived without disease progression [mean PFS: 32.9 months (range: 13.6–49)], which confirmed that ablation is a potentially curative strategy for selected patients with POs from HCC. Nakamura et al. [38] evaluated pulmonary metastasectomy in 30 patients with HCC. The 1-year, 3-year and median OS rates were 86.7%, 46.2% and 25.0 months, respectively. The study emphasized that use of the appropriate patient selection criteria was the key factor, namely, good general condition, fewer than 3 intrapulmonary metastatic tumors, stable or controllable intrahepatic tumors, limited to one lobe or one lung field, and no extrapulmonary tumors. Jeong YH [39] evaluated the outcomes of pulmonary metastasectomy in 52 patients after LT, and the 1- and 3-year OS rates were 75.0% and 43.5%, respectively, which indicated that a shorter recurrence-free period after LT and adjuvant treatment were independent risk factors. Our study showed that the 1-year, 3-year, and median OS rates were 98.4%, 43.7% and 33.0 months, respectively, which are superior to those obtained in Nakamura [38] and Jeong’s [39] studies. Moreover, the indications for ablation treatment are greater, the complications are fewer, the patient inclusion criteria are fewer, and cost-effectiveness is higher.
The most important finding of the study is that both the initial BCLC stage and treatments independently influence PFS and OS, which means that better PFS and OS can be obtained from initial evaluation and treatment strategies. Although the 29 (BCLC stage C) patients’ primary HCC was mostly controlled by TACE evaluated by enhanced CT, there may be living tumor tissue or HCC stem cells within or at the edge of the embolized zone, so radical treatments such as surgery or ablation are still needed to achieve complete biological necrosis rather than image necrosis. Jansen MC [40] reported that after TACE, a significant tumor response was achieved in 17-61.9% of patients, but a complete tumor response was rare (0-4.8%), as viable tumor cells remained after TACE confirmed by surgery. Frenette CT et al. [41] reported 111 patients with HCC who underwent cTACE (n = 76) or DEB-TACE (n = 35) before LT, and complete necrosis was achieved in 50.9% and 57.1% of cTACE and DEB-TACE confirmed by pathology, respectively. Chua TC et al. [42] showed that the pathological response of resected specimens was only 27–72% after TACE, although CR was demonstrated on images. Therefore, radical treatments for primary HCC, such as surgery, LT, or ablation, should be performed as soon as possible after TACE, even if CR is evaluated by CT or MR. It is not difficult to understand the impact of POs classification on PFS. Synchronous POs means that HCC cells have been transferred to the lungs through the blood system, and there should be free tumor cells in the circulatory system, which indicates a comparatively higher tumor burden than metachronous POs. That is to say, metachronous POs indicate isolated metastases after the primary lesion has been controlled, and are more suitable for local intervention. Such a phenomenon has been described at POs from lung cancer [43] and colorectal cancer [44] in previous studies. Child-Pugh class was not significant based on multivariate analysis (P = 0.11), although it showed significance in the univariate analysis, in contrast to previous studies [45]. The reason may be due to (1) the small sample (n = 19) of patients with Child‒Pugh > 5; (2) the improvement of albumin, ascites and other related indicators by conservative treatments; and (3) the fact that the Child‒Pugh class is only a stratification factor based on initial HCC diagnosis, and this indicator changed after surgery (n = 10) and LT (n = 4) in our study. Overall, this study confirmed that the thermal ablation used for POs is both feasible and safe, consistent with previous reports. It demonstrated that thermal ablation for POs can achieve significantly better survival outcomes than historical data (especially those based solely on supportive treatment or systemic treatment), and it also has the advantage of being minimally invasive.
In conclusion, the study supported the ablation of POs from HCC with good results, and initial BCLC stage evaluation and treatment strategies should be emphasized in our future practice. Given the limitations of this article including a small sample size, retrospective design, single-center data, and selection bias. In the future, multi-center prospective studies need to be conducted to verify the long-term efficacy of thermal ablation in POs and to explore the optimization strategies for combined systemic treatments.



Comments (0)