
Remember me


Our study design was approved by the ethics review committee of China-Japan Friendship Hospital. All patients provided written informed consent to undergo simultaneous percutaneous CT-guided biopsy and cryoablation as part of their clinical care. This retrospective pilot study included 124 patients from December 2020 to May 2024. Patients who underwent percutaneous core-needle biopsy and cryoablation simultaneously were classified as Group A, whereas those who had these procedures performed separately were classified as Group B, with an interval of more than one week between the core-needle biopsy and cryoablation. The pathology was obtained by biopsy prior to cryoablation in these Group B patients. The inclusion criteria were as follows: Patients with pulmonary nodules ≤ 3 cm that were highly suspicious or already confirmed as malignant, indicated by signs such as lobulation, pleural indentation, bronchial inflation, vascular bundle involvement, or diameter enlargement during follow-up. These assessments were confirmed by multidisciplinary teams from the thoracic, respiratory, pathology, and radiology departments [11, 12]. Both core-needle biopsy and cryoablation had to be performed either synchronously or separately. Patients were deemed unsuitable for surgery due to multiple previous surgeries, advanced age, impaired lung function, or personal refusal. Exclusion criteria included: Severe coagulation disorders and an extremely poor health condition that prevented cooperation with medical staff.
Technique proceduresPrior to the procedure, a pre-procedural CT scan was conducted to evaluate tumor characteristics and plan the cryoablation approach. This assessment included tumor size, location, proximity to critical structures, and the determination of the number of cryoablation probes required. Anticoagulant or antiplatelet medications were discontinued before the operation. Patients were positioned in the prone, supine, or lateral position, depending on the lesion’s location. The procedure was performed by two experienced interventional radiologists, each with 10 to 15 years of experience, using a 16-detector-row scanner (Aquilion 16; Canon Medical Systems) and argon and helium gas as cryogens. The technical parameters included: (1) scanning method: helical acquisition mode; (2) tube currents: automatic tube current modulation; (3) tube voltage: 120 kVp; and (4) slice thickness: 4–5 mm. Only the lesion area was scanned to minimize radiation exposure.
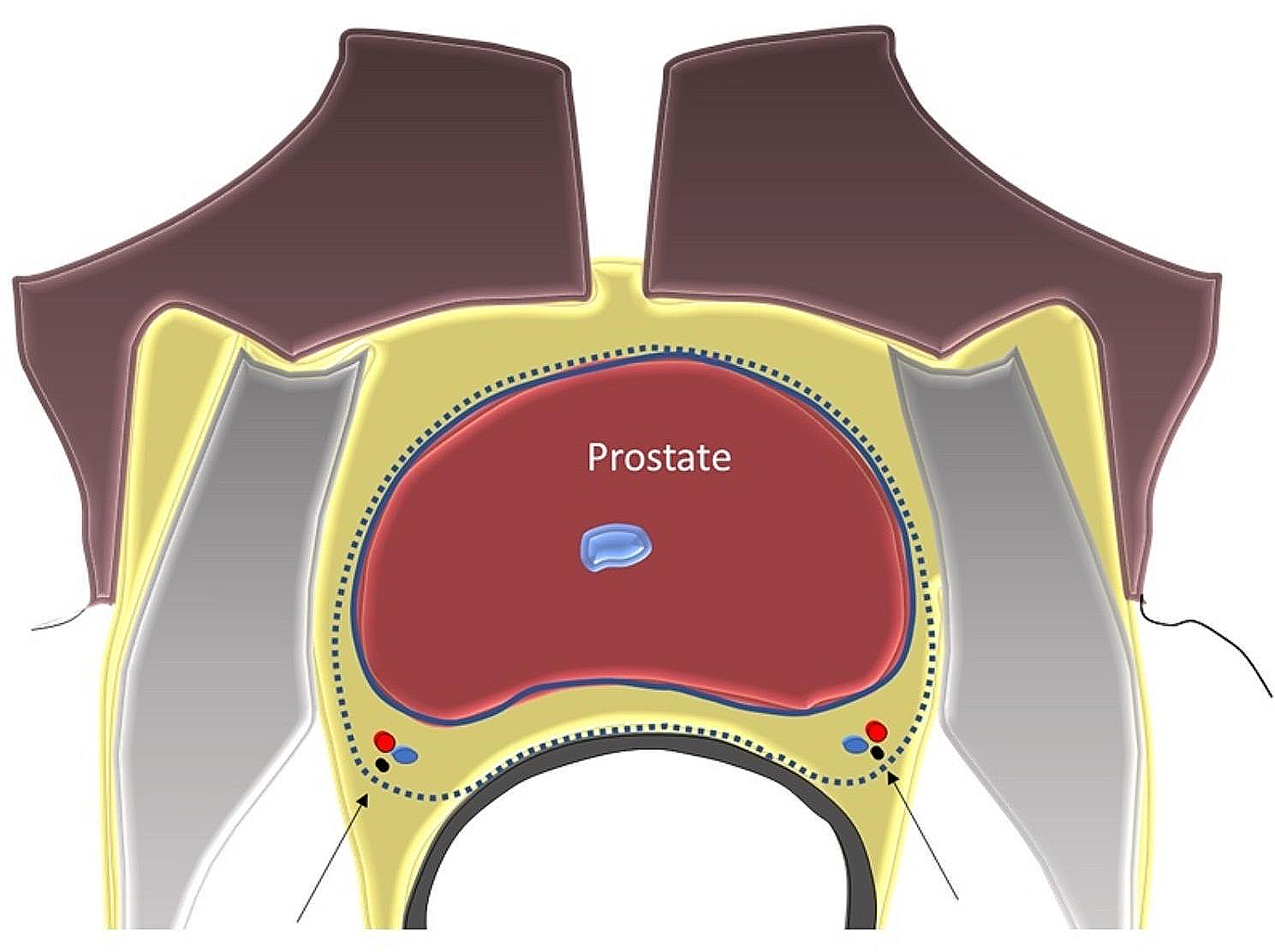
The biopsy system consisted of an introducer needle and an 18G or 20G core biopsy instrument (Argon Medical Devices, Inc., Athens, TX). The operators selected the appropriate approach to the lesion based on imaging to ensure the shortest puncture pathway while avoiding critical structures such as large blood vessels, bronchi, and interlobar fissures. Local pleural anesthesia was administered using 5 ml of 1% lidocaine. A 6.8 cm-long, 1.7 mm-diameter percutaneous introducer needle was advanced from the marked skin point, ensuring it did not penetrate the parietal pleura. Once the needle was positioned within the target lesion, two to three specimens were collected using the core biopsy instrument for subsequent histological evaluation and diagnosis. Before cryoablation, we performed a preoperative integrity test of the cryoprobe in a saline solution to confirm its functionality and rule out the possibility of argon leakage. Cryoprobes (Endocare, Irvine, California) were then inserted into the target area parallel to the lesion, maintaining a distance of less than 0.5 cm between the probe and the nodule’s edge (Fig. 1). A double-probe method was employed in cases where a single probe could not achieve complete ablation. This technique created a “clamping freezing” effect, allowing both cryoprobes to deliver energy from either side of the tumor, ensuring comprehensive coverage by the ablation zone for optimal results [13].
Fig. 1
Synchronous biopsy and cryoablation procedure. The yellow needle is the core biopsy instrument, and two white needles are cryoablation probes
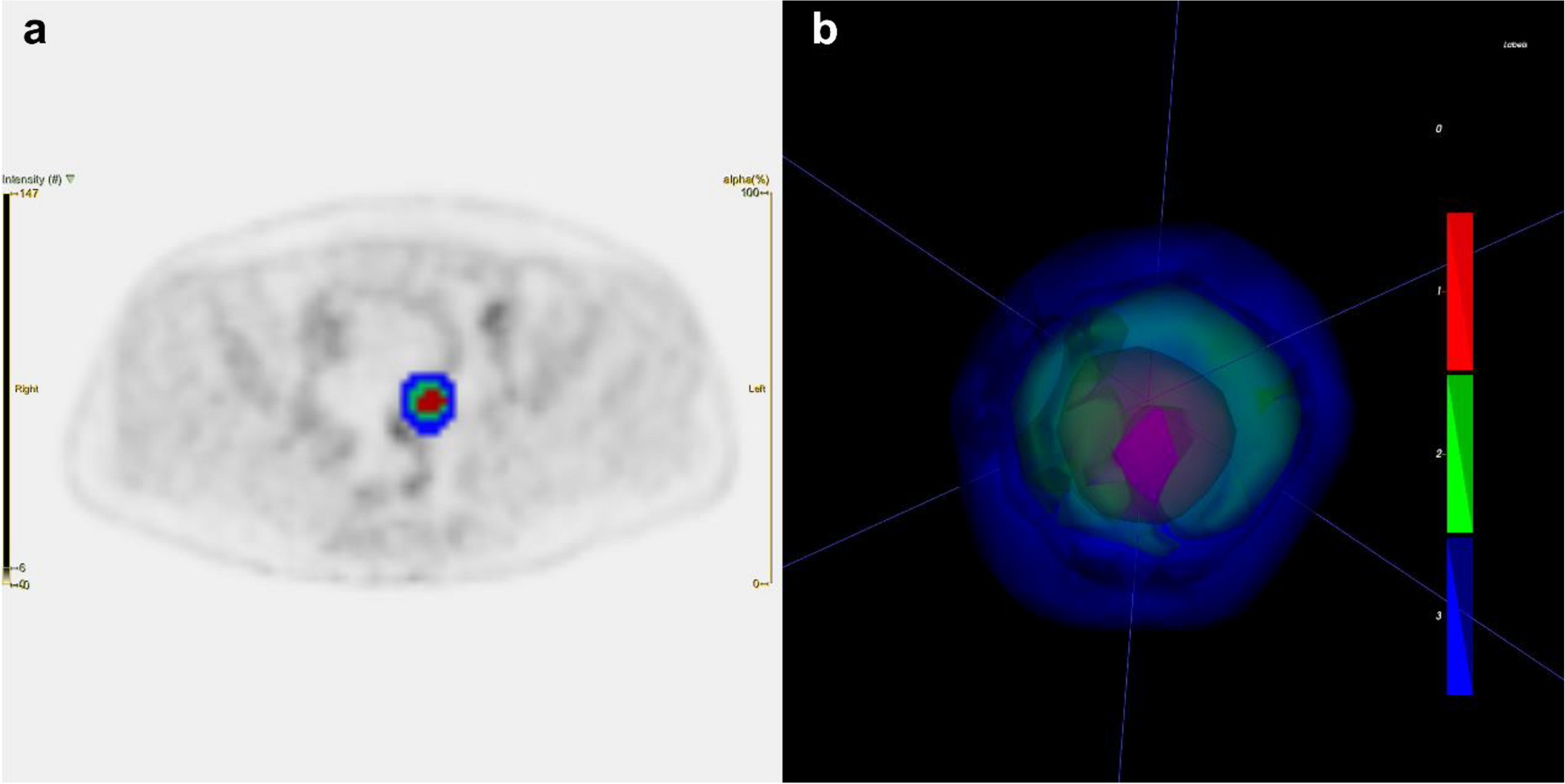
Cryoablation involved rapidly cooling the tissue using argon gas, which formed an ice ball around the tumor [14]. Two or three freezing-thawing cycles were applied, with each freezing cycle lasting 10 to 15 min, interspersed with a five-minute heating session with helium. The total freezing time was 30 min. Real-time CT imaging was performed every five minutes to assess the ice ball’s formation. The edge of the ice ball was maintained at least 1.0 cm larger than the tumor’s edge to ensure complete ablation and satisfactory clinical outcomes (Figs. 2 and 3).
Fig. 2
Synchronous procedure in a 71-year old woman. (a) Computed tomography image showing a single sub-solid nodule (arrow), 20 mm ×12 mm, in the apical segment of the right upper lobe, irregular margin, and pleural tail sign. (b) A cryoablation probe (long arrow) was placed into the nodule while the biopsy needle was at the edge of the lesion (short arrow). (c) During the cyroablation procedure, the locus center began to occur liquefactive necrosis as well as the ice ball emerged (arrows). (d) In the thoracic computed tomography scan immediately after cryoablation, the ablated nodule presented with a circular ground-glass opacity (arrow). Finally, the pathological result showed it an early stage lung adenocarcinoma
Fig. 3
Synchronous procedure in a 77-year old woman. (a) Computed tomography image showing a single solid nodule (arrow), 11 mm ×6 mm, in the apical segment of the right superior lobe, regular margin, with pleural tail sign. (b) A cryoablation probe (long arrow) was placed into the nodule while the biopsy needle was at the edge of the lesion (short arrow). (c) During the cyroablation procedure, the locus center began to occur liquefactive necrosis as well as the ice ball emerged (arrows). (d) In the thoracic computed tomography scan immediately after cryoablation, the ablated nodule presented with a circular ground-glass opacity (arrow). Eventually, the pathological result showed it a lung adenocarcinoma
In Group B, patients diagnosed with primary lung cancer or metastases after biopsy subsequently underwent percutaneous cryoablation once any complications from the biopsy were resolved. The technical aspects of the biopsy and cryoablation in this group were similar to those in the synchronous procedure.
Post-procedural care and follow-upAfter cryoablation, patients were monitored in a recovery area for a specified period. Post-procedural CT scans were conducted to assess the immediate technical success of the cryoablation procedure, ensuring that the edge of the ice ball was 0.5–1 cm larger than the tumor’s edge to confirm complete ablation. These scans also aimed to detect any immediate complications, such as pneumothorax, hemorrhage, pleural effusion, and other adverse events [15].
Treatment-related complications were evaluated according to the Society of Interventional Radiology criteria [16, 17]. The primary complications included pneumothorax, hemoptysis, and pleural effusion. Major complications are life-threatening and necessitate prolonged hospitalization, while minor complications are self-limiting and typically require only a short hospital stay for observation or treatment.
The degree of pneumothorax was classified as severe (lung compression > 50%), moderate (lung compression ≤ 50% and > 20%), and mild (lung compression ≤ 20%). Hemoptysis was categorized as severe (> 100 mL), moderate (10–100 mL), and mild (≤ 10 mL). Pleural effusion was classified as severe (> 1000 mL), moderate (500–1000 mL), and mild (≤ 500 mL).
Follow-up observations included pathological results, the technical success rate, and the local tumor control rate. Local tumor progression (LTP) was identified by an increase in the ablation zone size compared to the baseline CT scan performed one month after cryoablation, accompanied by irregular, scattered, nodular, or eccentric enhancement, or circumferential expansion during imaging follow-up [18].
Data collection and statistical analysisDemographic data of the enrolled patients, characteristics of pulmonary nodules, procedural details, complications, and efficacy rates per nodule were collected for statistical analysis. All parameter values were tested for normality and homogeneity of variance. Continuous variables were expressed as mean ± standard deviation for normally distributed data and median ± interquartile range for non-normally distributed data. Differences between the synchronous and separate procedures were analyzed using Pearson’s Chi-squared test or Fisher’s exact test for categorical variables. A p-value of < 0.05 was considered statistically significant. All analyses were conducted using SPSS software version 25.0.
Comments (0)