In-vitro studySensory neuron differentiation
Two human iPSC lines from healthy donors were obtained commercially (A18945, ThermoFisher, Roskilde, Denmark, hpscreg.eu/cell-line/TMOi001-A; WTC-11, Gladstone Institute of Cardiovascular Disease, University of California San Francisco, hpscreg.eu/cell-line/UCSFi001-A). The iPSCs were maintained, passaged, and differentiated into sensory neurons as previously described and confirmed in detail [21]. Briefly, iPSCs were maintained in mTeSR1 medium (85850, StemCell Technologies, Vancouver, BC, Canada) on Matrigel-coated 6-well plates (354277, Corning, NY, USA) at a minimum density of 50,000 cells/cm2. The medium was changed daily, and iPSCs were routinely passaged at ∼70–80% confluency using Accutase (00455556, ThermoFisher). The differentiation was performed using 5 small molecule inhibitors for 12 days, followed by maturation with four neurotrophic growth factors and ascorbic acid (A4403, Sigma-Aldrich, Saint Louis, MO, USA) for an additional 23–33 days. On day 12, immature sensory neurons were seeded as single cells at a density of 150,000 cells/cm2 on culture plates coated with poly-L-ornithine hydrobromide (20 µg/mL, P3655, Sigma-Aldrich), laminin (10 µg/mL, 23017015, ThermoFisher), and fibronectin (2 µg/mL, F1141, Sigma-Aldrich). On day 14, non-neuronal cells were removed using Mitomycin-C (1 µg/mL, M4287, Sigma-Aldrich) for 2 hours. On day 16, all medium was replaced; afterwards, 50% of the medium was changed every 3–4 days. The mature sensory neurons were used for experiments between days 35–45.
Chemotherapy exposure
Oxaliplatin (O9512, Sigma-Aldrich) was dissolved and serially diluted in sterile water. The final concentration of sterile water was maintained at 0.2% for all conditions, and the same concentration of sterile water was included as a control. The concentrations of oxaliplatin were chosen based on the maximum plasma concentrations observed in clinical pharmacokinetic studies and adjusted to account for the inability to carry out repeated oxaliplatin exposure [22]. After 96 h of exposure to oxaliplatin, the medium was collected, and the respective iPSC-derived sensory neurons (iPSC-SNs) were lysed using radioimmunoprecipitation assay buffer (89900, ThermoFisher).
Immunolabeling
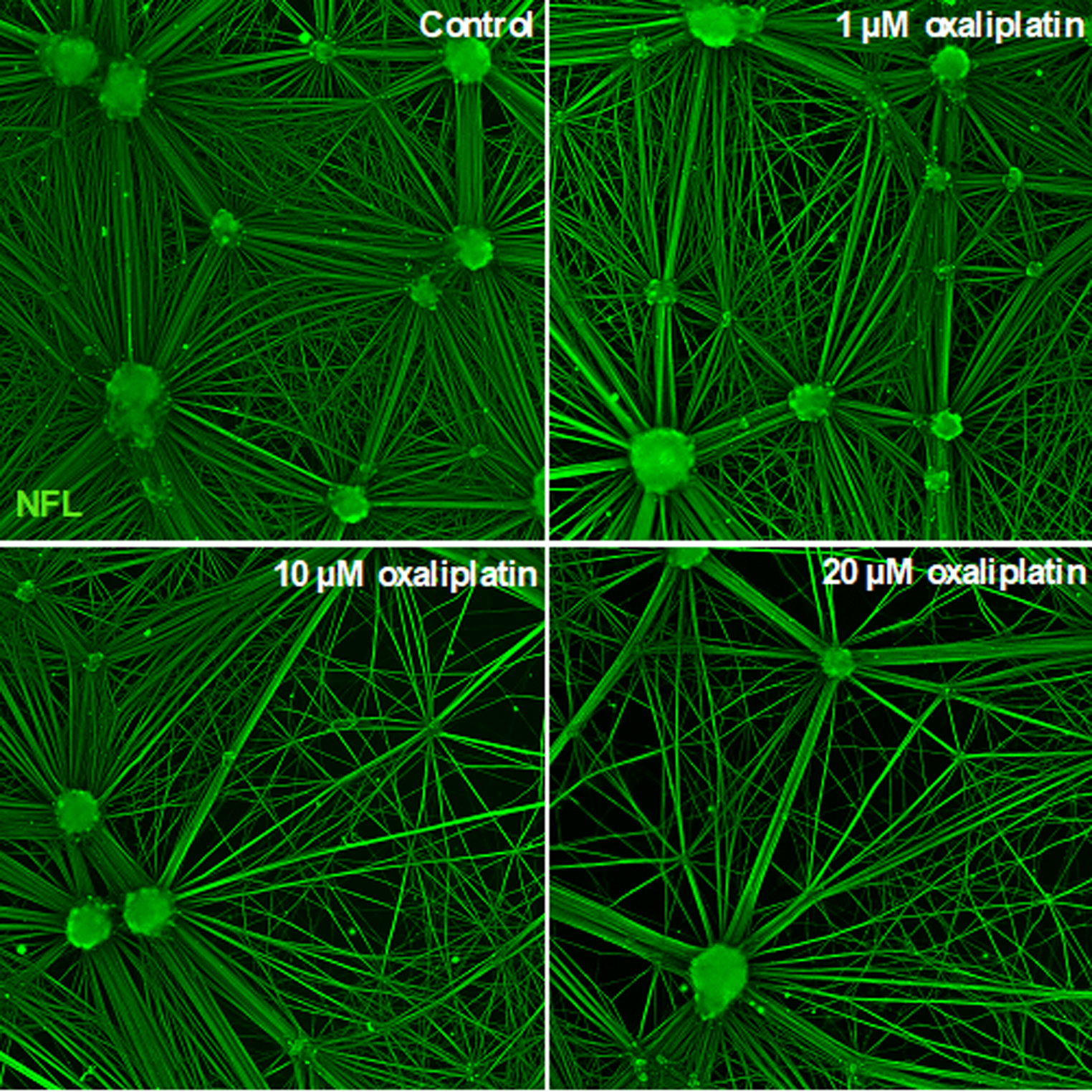
Human induced pluripotent stem cell-derived sensory neurons (iPSC-SNs) were fixed with 4% paraformaldehyde for 10 min, washed twice with phosphate-buffered saline (PBS, D8662, Sigma-Aldrich), and subsequently permeabilized with 0.25% Triton X-100 for 15 min. An unspecific binding was subsequently blocked using 1% bovine serum albumin (A9418, Sigma-Aldrich) for one hour. iPSC-SNs were labeled with NFL monoclonal antibody (1:100, MA5-14981, ThermoFisher) overnight at 4 °C. The following day, iPSC-SNs were labeled with Alexa Fluor 488-conjugated anti-rabbit (1:400, A11008, ThermoFisher) for 1 h at room temperature. Images were acquired using ImageXpress Pico Automated Imaging System with the 10X objective (Molecular Devices, San Jose, CA, USA).
Analysis of cell data
iPSC-SN experiments were performed for two individual donors with three technical replicates per condition. NfL levels were adjusted for protein concentrations, and fold changes in NfL levels were calculated relative to the mean value of the vehicle control for each individual differentiation.
Clinical study
From 2019 to 2021, patients diagnosed with colon cancer seen in the Department of Oncology, Vejle Hospital, and University Hospital of Southern Region of Denmark were invited to participate in the study. Eligible participants were adult patients aged 18–90 with a diagnosis of colorectal cancer stage III or IV. Patients followed treatment regimens according to clinical guidelines, which led to the formation of two groups based on whether their regimen included oxaliplatin. An oxaliplatin regimen comprised a minimum of four planned treatment cycles of oxaliplatin (130 mg /m2) in combination with capecitabine (2000 mg/m2) every three weeks. The non-oxaliplatin treatment regimens comprised eight planned treatment cycles of capecitabine (2000 mg/m2) every three weeks or a treatment regimen including folinic acid, fluorouracil, and irinotecan every two weeks. Exclusion criteria for both groups were a history of oxaliplatin treatment, lumbar radiculopathy, lower extremity peripheral neuropathy, or peripheral vascular disease. Patients were evaluated prior to treatment, after 3 months, and after 6 months. These visits coincided with the patient’s oncological treatment schedule, with the 3-month evaluation occurring approximately at the 5th treatment cycle and the 6-month evaluation around the 8th cycle. At each visit, OIPN evaluation and blood sampling were carried out.
OIPN evaluation
An oncologist evaluated the symptoms of OIPN in an interview, including dichotomized presence of the following symptoms in each lower extremity: numbness, pricking sensation, pain, muscle weakness, and ataxia. Each positive answer generated one point resulting in a combined score of both extremities ranging from 0 to 10. We defined possible OIPN as the bilateral presence of numbness and/or presence of pricking sensations in the feet as previously done [1, 3], correlating to the score of minimum 2 on the transformed possible OIPN grading scale.
Information on treatment modality accumulated oxaliplatin dosage, the reason for dose reduction and premature cessation, and certain comorbidities were obtained from patient records from the oncological department during the treatment period.
Blood sampling
Blood samples (10 mL) were collected by venous puncture and drawn into serum tubes according to standard procedure. After allowing the blood to coagulate for 30 min, the samples were centrifuged at 2,000 g for 10 min. The supernatant was then stored at -80 °C until use.
NfL analysis
NfL measurements of iPSC-SN medium and patient serum were conducted at the Department of Biochemistry and Immunology, University Hospital of Southern Denmark, Vejle, Denmark. Measurements were performed blinded to experimental and clinical data using a commercially available NfL assay on the Single molecule array (Simoa®) HD-X Analyzer (Quanterix, Billerica, MA, USA). iPSC-SN medium samples were diluted 100-fold in buffer included in the assay kit and analyzed in duplicates. Serum samples were diluted four-fold in the buffer and analyzed as single determinations. Quality control was performed using two controls prepared from commercially available control material provided by the manufacturer in addition to an in-house prepared serum pool. The quality controls were included in each run for evaluating and monitoring assay performance. The analytical coefficients of variation were below 13%.
Study approval and statement of human and animal rights
The protocol was approved by the Ethical Committee of the Southern Region of Denmark (S-20190048 approved Aug 5th, 2019). Patients provided written and informed consent before enrolment in the study. The study is non-interventional and collected data was anonymized.
Statistics
Descriptive statistics were used to describe patient demographics in the two groups. Numerical data were analyzed using Wilcoxon rank-sum test due to non-normal distribution. Linear mixed model analysis was used to estimate the predicted levels of NfL and possible OIPN score in the two groups and visualized using margin plots. Relevant adjustments were determined using directed acyclic graphs (DAGs), and age and diabetes were adjusted for [23]. Post-estimation Wald test was used to determine statistically significant different levels between repeated measurements. The mixed model took missing values into account.
Linear regression evaluated the association between accumulated oxaliplatin dose and NfL and possible OIPN score at different time points, including only complete cases. The correlation between NfL and possible OIPN score was calculated using Spearman correlation and linear regression. Statistical significance level was determined to be α = 0.05. Data analysis was carried out in STATA/SE version 18.

Comments (0)