This sample is comparable to other populations described in the literature like Osbeck et al. [13].
The clinical scores in our series showed a significant improvement after the surgery, with an AOFAS score of 83.66 and an EFAS score of 20.08. Myerson et al. reported similar values, with an AOFAS score of 79 points [5].
There was no significant improvement in clinical scores between groups when the calcaneal translation was greater than or equal to 10 mm as compared to a 7.5 mm translation achieved with Step Plate® plates.
In this study, six patients were unsatisfied with the surgery, with AOFAS scores below 70 points and EFAS scores below 16, representing 14% of our series. Persistence of pain and associated functional limitations were the main reason for patients’ dissatisfaction with the surgical outcome. Myerson et al. in 2002 reported an 8% dissatisfaction rate post-operatively for similar reasons [5]. Fayazi et al. reported that two patients (9%) did not improve: one due to a work-related injury and the other due to deep vein thrombosis with residual leg oedema.
Among our six dissatisfied patients, one experienced a recurrence of the flatfoot valgus deformity, while another showed no correction of a significant deformity, with a calcaneal valgus of 14° and a talus–M1 angle of 16° pre-operatively. A third patient is being treated for chronic pain in the operated limb. For the remaining patients, no obvious cause for the persistent pain was identified, which does not appear to be related to iatrogenic sural nerve damage or ankle osteoarthritic deterioration.
At the last follow-up, radiographic parameters remained unchanged from those recorded immediately post-operatively. These results are consistent with the study by Niki et al. in 2012 [3], which highlighted the persistence of radiographic changes between the immediate post-operative period and the final follow-up. However, they noted a loss of correction in patients with a calcaneal valgus > 15°, who also had poorer functional scores. In our study, only six patients had such a valgus, and no significant differences were found between the two groups. However, we observed that these patients had the least satisfactory scores, with under-correction or recurrence of the deformity, even though the intraoperative translation performed was 7.5–10 mm.
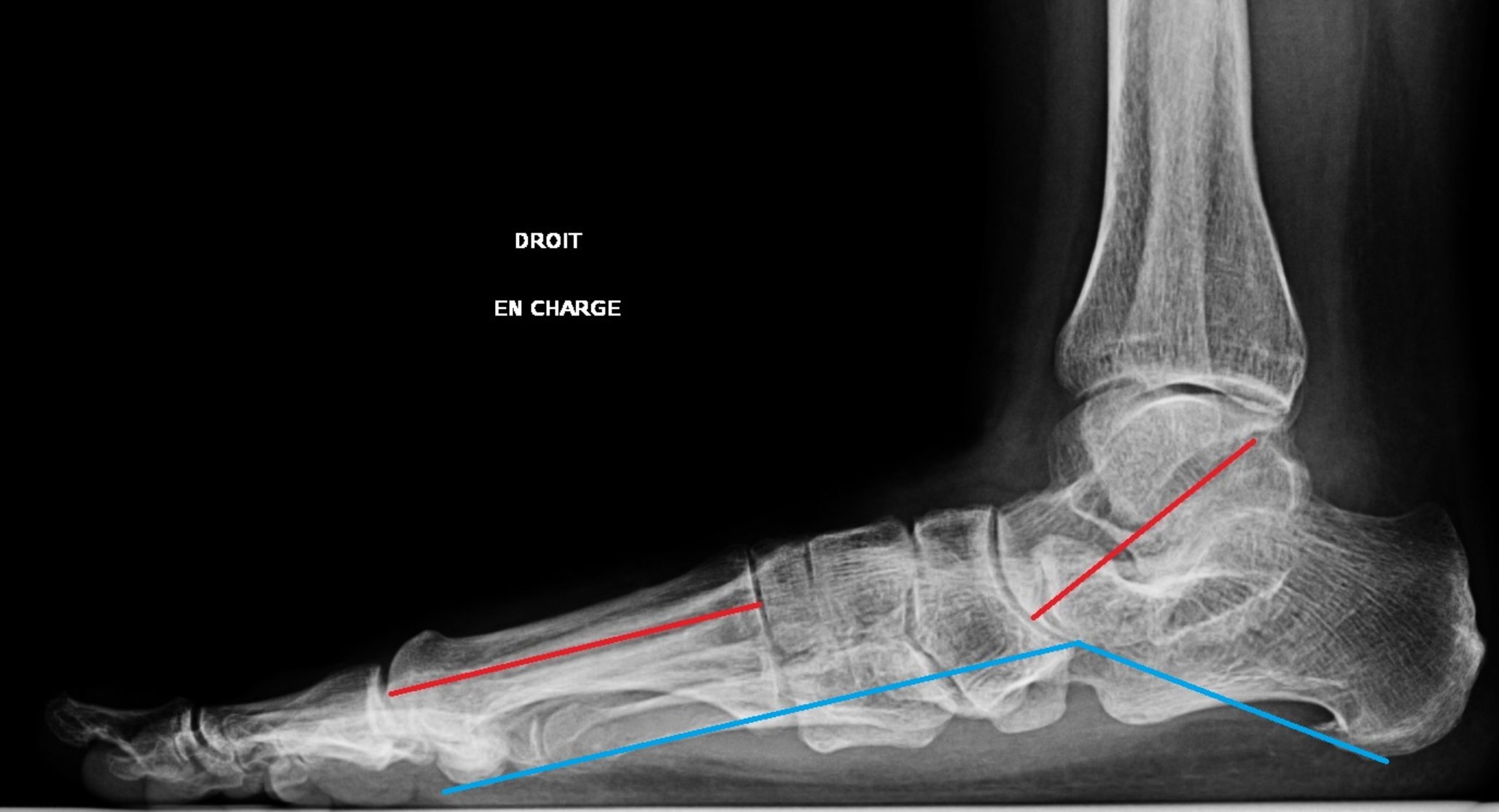
A pre-operative lateral talus–M1 angle greater than 25° is associated with poorer long-term outcome [3]. None of our patients presented with such a deformity, which probably supports a better pre-operative selection, excluding Myerson medialization osteotomy in the most severe cases.
We did not find any correlation between pre- or post-operative radiographic measurements and the clinical outcomes reported by the patients. This observation aligns with literature data from Niki and Sammarco on Myerson osteotomy, which does not significantly modify the structural parameters of the foot [3, 14].
When analyzing patients by the tendon transfer status, the demographic groups were similar apart from age. Patients who underwent a transfer were older than those who did not (49.3 vs. 56.3, p = 0.024).Post-operatively, the clinical outcomes were comparable between the groups with and without tendon transfer. DiDomenico et al. previously reported that satisfactory results could be achieved without tendon transfer, but the surgical technique described combined a double calcaneal osteotomy, first column stabilization, and gastrocnemius lengthening [15].
Radiographically, the minimal impact of tendon transfer on arch correction is well-known, with structural changes mainly attributed to the osteotomy [4, 16].
In 2007, Bolt compared calcaneal medialization and lengthening osteotomies, demonstrating a greater and more lasting correction with lengthening, but at the cost of increased adjacent joint osteoarthritis and more frequent nonunion. To the best of our knowledge, no studies have employed a follow-up period as lengthy as that observed in isolated medialization osteotomies with or without tendon transfer.
The combination of lengthening and medialization osteotomies has been suggested by some authors to correct both heel valgus and forefoot abduction, especially when talar uncovering exceeds 30° [17, 18]. The available two year results are favorable, with an AOFAS score around 80 and a restoration of medial arch height on radiographs [18].
Osman et al. reported that hardware discomfort was the main reason for reoperation, which was performed in 26% of their patients [19, 20]. In our series, the reoperation rate was lower, with only 15% requiring hardware removal, with no difference between plates and screws.
Six patients experienced pain during clinical examination of the subtalar joint, raising concerns about potential osteoarthritic degeneration. However, this degeneration appears to be relatively well-tolerated, as none of the patients had sought specific treatment for these pains, such as corticosteroid injections.
In the two published series with follow-ups of more than ten years concerning medialization osteotomy, the reoperation rate was low. In Ruffilli’s series of 90 medialization osteotomies, four failures (4.5%) required revision surgery with subtalar arthrodesis [21]. Chadwick et al. also noted four failures (12%), defined as a recurrence of pain and loss of function requiring revision surgery.
To date, none of our patients has required revision surgery for hindfoot arthrodesis, which is the alternative to conservative treatment with calcaneal osteotomies [22, 23].
Ivanic and al. and Gonzalez-Martin and al. report a neurological complication rate between 7% and 35% [24, 25].
The development of percutaneous surgery could lower neurological complications, but there is a discrepancy on this point in the literature [26,27,28]. Wayzi et al. in 2018 showed a shorter operating time, but similar X-ray irradiation and no significant difference in the clinical outcome.
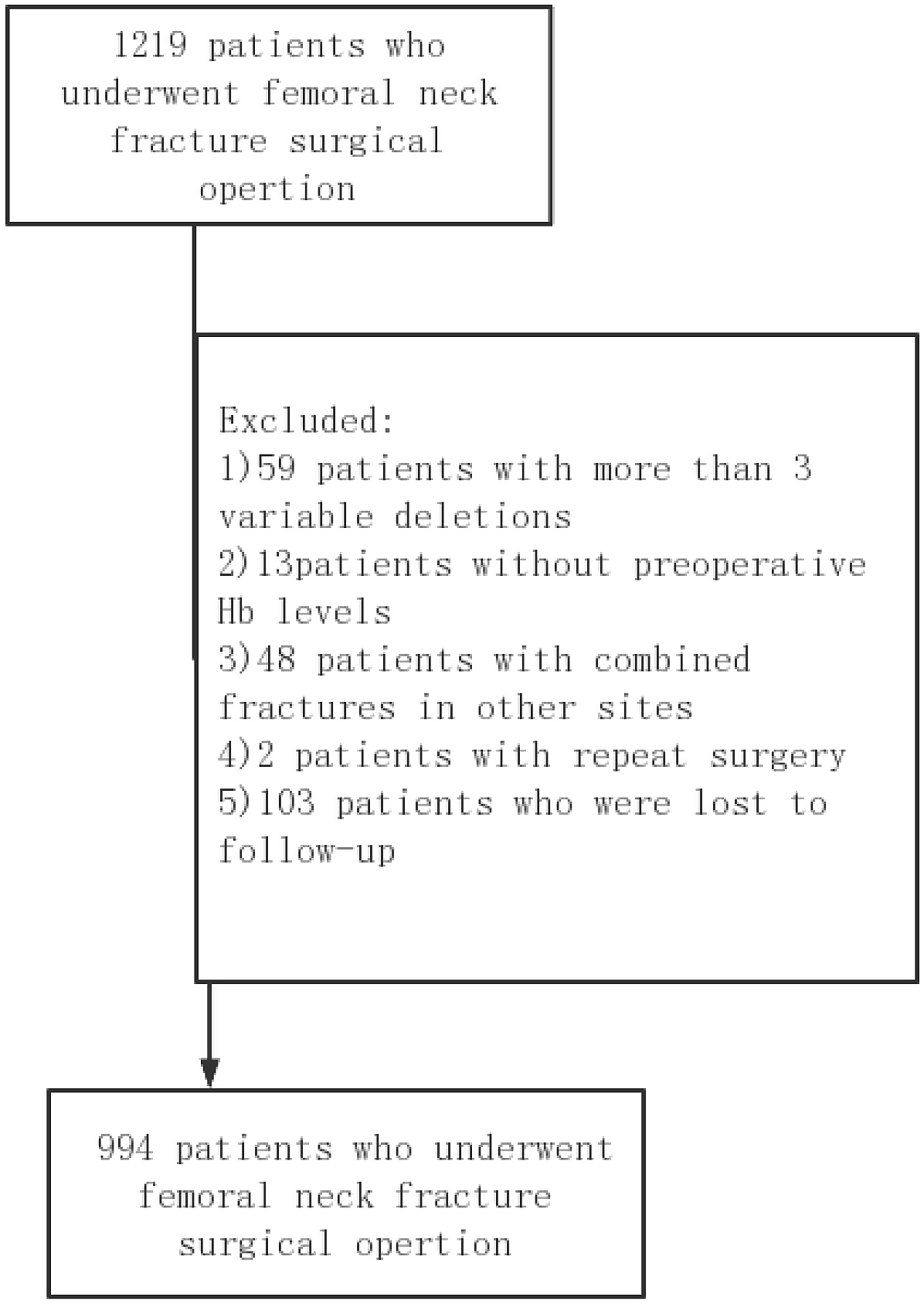
In this study almost 40% of the initial operated patients were lost to follow up over five years, but given this long term this figure can be considered as acceptable [29].
Regarding the analysis of radiographic parameters, we must note the absence of an evaluation of the talo-navicular divergence on the weight-bearing anteroposterior foot radiograph. This parameter is frequently assessed as midfoot abduction; however, the lack of systematic preoperative imaging made it impossible to compare findings before and after surgery.



Comments (0)