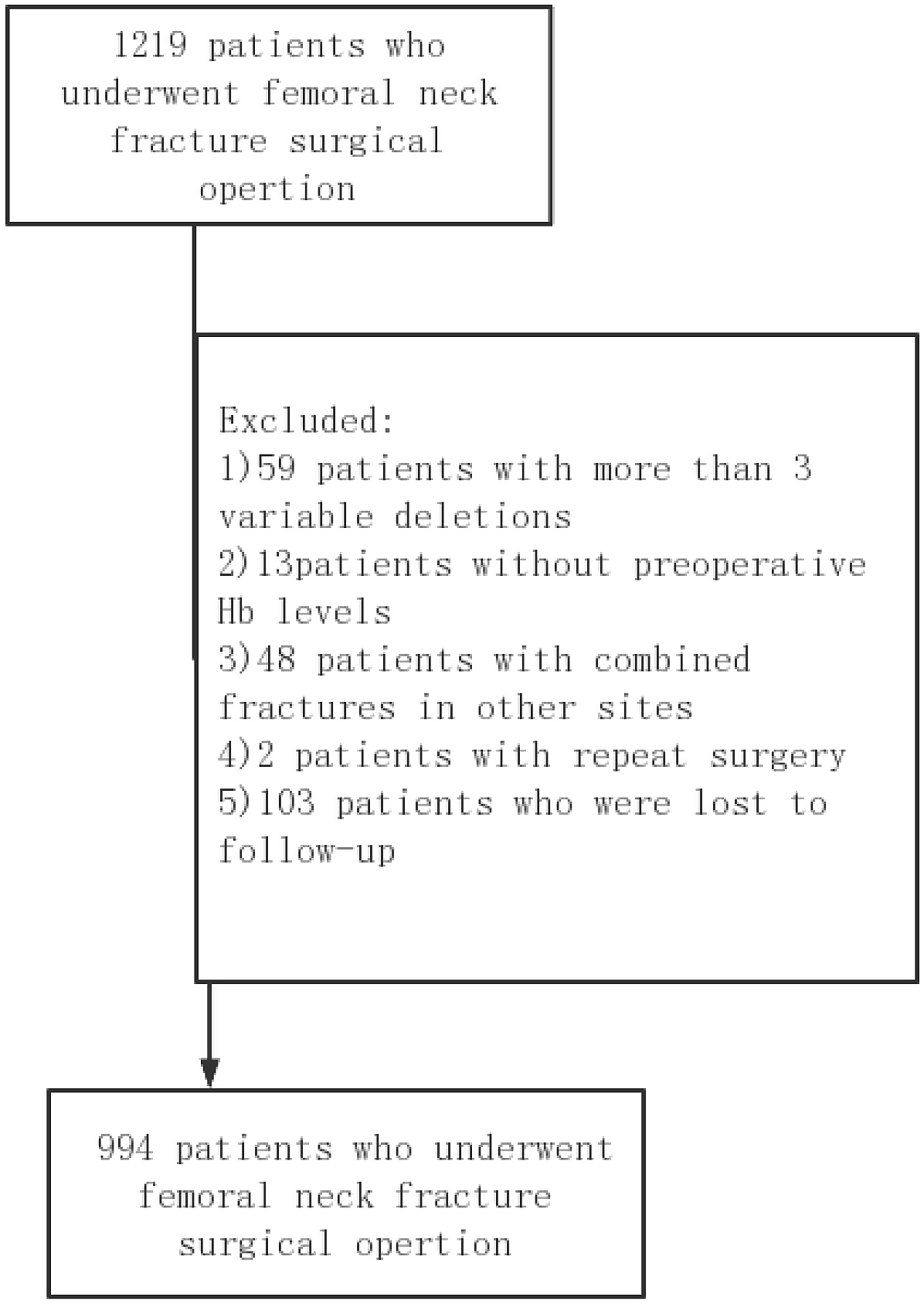
A detailed retrospective cohort analysis was conducted at our medical centre, involving 994 consecutive patients who underwent elective unilateral primary fixation for femoral neck fractures (FNF). The study revealed a one-year mortality rate of 8.45%, notably lower than the previously reported range of 15–50% for similar procedures [23–24]. In contrast, the postoperative mortality rate for internal fixation patients in our study was 0%. This difference may be attributed to the fact that our study population was composed of individuals aged over 60 years, with exclusion criteria that eliminated high-energy trauma cases and revision surgeries. Additionally, the standardized perioperative protocol at our institution may have contributed to the lower mortality rate observed. We acknowledge the potential for selection bias, which represents a limitation of the study, and recommend that further multicenter studies be conducted to validate these findings. Furthermore, internal fixation patients were younger (mean age: 65.24 ± 5.43 vs. 79.33 ± 7.46 for hemi-hip replacement) and had lower ASA scores (89.58% vs. 50.54% for hemi-hip arthroplasty) (as shown in Attached Table 1). These factors may have contributed to the more favourable postoperative recovery. The variability in mortality rates observed in previous studies emphasizes the challenges of drawing definitive conclusions without comprehensive data stratification and analysis. The presence of multiple confounding risk factors further complicates the evaluation, necessitating a more detailed approach to assess the impact of each identified risk factor on patient outcomes.
Effective perioperative management is crucial in determining outcomes such as postoperative complications and mortality rates. Nevertheless, a significant number of research studies focused on mortality following femoral neck fractures have neglected to thoroughly explore the nuances of perioperative strategies and their subsequent effects. Our research highlights that moderate to severe anaemia in male patients significantly forecasts increased postoperative mortality. Particularly, this condition correlates strongly with other severe health issues like hypertension (odds ratio [OR] = 3.49, p = 0.0092), coronary heart disease (OR = 4.00, p = 0.0095), an ASA score of 1 (OR = 3.52, p = 0.0437), and the necessity for multiple units of blood during surgery (OR = 17.97, p = 0.0065). This aligns with findings from Kastanis et al., which identified ASA status as a prognostic marker for medical complications and hospital readmissions in geriatric patients with hip fractures [26]. Although our study employed a stratified analysis to delve deeper into these associations, it is noteworthy that such detailed stratifications are often under reported in the literature.
In the observed study, 221 patients exhibited moderate to severe anemia, while 486 presented with mild anaemia, and 287 displayed no signs of anaemia. Research conducted by Zhang Hui and colleagues [27] identified the prevalence of preoperative anaemia among patients suffering from femoral and pelvic fractures as 47.8%. However, in our analysis, the prevalence rate escalated to 75.2% among individuals with femoral shaft fractures, indicating a higher occurrence rate of preoperative anaemia at this specific anatomical site.The impact of anaemia on the likelihood of mortality within one year following femoral neck fracture surgeries in the elderly population showed variability. Specifically, among elderly patients suffering from hip fractures, those identified with anaemia—defined as haemoglobin concentrations below 12.0 g per deciliter for female patients and below 13.0 g per deciliter for male patients—demonstrated a higher probability of being nonambulatory at the time of hospital discharge when contrasted with their non-anaemic counterparts [28]. Contrarily, another study noted no significant variance in the recovery levels regarding ambulation or daily living activities at three, six, or twelve months post-surgery between anaemic and non-anaemic subjects [29]. An earlier study highlighted that while admission haemoglobin levels correlated with mobility on a univariate scale, this correlation faded under multivariate analysis [30]. The lack of significant outcomes across these studies could stem from the differing anaemia severity levels among participants. It is revealed through our investigation that only moderate to severe anaemia has a consistent impact on the risk of mortality within a year, while the influence of mild anaemia appears more subdued. Neglecting to identify and address preoperative anaemia promptly can lead to a surge in blood transfusions, an increased risk of infections, higher residual rates, and elevated mortality rates, alongside prolonged hospitalization durations and diminished postoperative functionality. Even mild anaemia can significantly heighten the risk of developing these complications [31–32].
Our investigation established that for patients experiencing moderate to severe anaemia, a rise of 1 g/dL in preoperative haemoglobin (Hb) levels is linked to an approximately threefold (2.96 times) increase in the likelihood of mortality within the subsequent year. This strong association persists robustly after controlling for confounding factors such as age, gender, blood pressure, and pre-existing coronary conditions, highlighting preoperative anaemia as a potent independent predictor of mortality risk. Further investigations corroborate these findings, showing that mild anaemia at the time of admission is linked to a 50% increase in mortality within three months (95% CI: 1.1–1.9). The risk escalates with the severity of anaemia; moderate anaemia correlates with a 2.6 times higher risk (95% CI: 2.0–3.4), and severe anaemia corresponds to a 3.6 times increase (95% CI: 1.8–6.9) in mortality compared to individuals without anaemia [33]. These data are particularly relevant to healthcare systems in China, where demographic patterns, such as an aging population, can influence outcomes. Our study also found that age is a risk factor for postoperative death in elderly femoral neck fracture patients, with the risk increasing with age. A critical age threshold of 76 years was identified, with a significantly increased risk of death after this age, as confirmed in other studies of Bzovsky et al. [34]. This increased in risk may be due to the decline in bodily functions, weakening of immune tolerance, and reduced self-healing abilities, leading to an increased risk of complications and eventually increased mortality. Haemoglobin levels prove to be a vital, cost-effective metric for predicting mortality among elderly patients who suffer from femoral neck fractures. Leveraging this prognostic factor could substantially improve healthcare outcomes. However, it is pertinent to note that our study did not delve into analyzing the specific causes of death, which could provide further insights into the correlations observed.



Comments (0)